

Genetically abnormal circulating cells in lung cancer patients: an antigen-independent fluorescence in situ hybridization-based case-control study
- PMID: 20651054
- PMCID: PMC2949278
- DOI: 10.1158/1078-0432.CCR-09-3358
Genetically abnormal circulating cells in lung cancer patients: an antigen-independent fluorescence in situ hybridization-based case-control study
Abstract
Purpose: We performed a study to determine if a fluorescence in situ hybridization (FISH)-based assay using isolated peripheral blood mononuclear cells (PBMCs) with DNA probes targeting specific sites on chromosomes known to have abnormalities in non-small cell lung cancer (NSCLC) cases could detect circulating genetically abnormal cells (CACs).
Experimental design: We evaluated 59 NSCLC cases with stage I through IV disease and 24 controls. PBMCs and matched tumors were hybridized with 2 two-color [3p22.1/CEP3 and 10q22.3 (SP-A)/CEP10) and 2 four-color [CEP3, CEP7, CEP17, and 9p21.3 (URO); and EGFR, c-MYC, 6p11-q11, and 5p15.2 (LAV)] FISH probes. Percentages of cytogenetically abnormal cells (CACs) in peripheral blood and in matched tumor specimens were quantified by using an automated fluorescent scanner. Numbers of CACs were calculated based on the percentage of CACs (defined as PBMCs with genetic abnormalities) per milliliter of blood and expressed per microliter of blood.
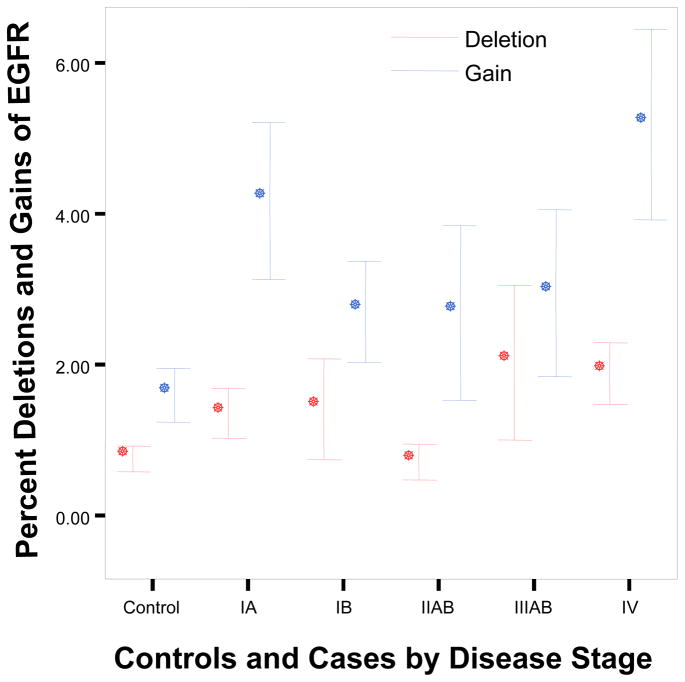
Results: Patients with NSCLC had significantly higher numbers of CACs than controls. Mean number of CACs ranged from 7.23 +/- 1.32/microL for deletions of 10q22.3/CEP10 to 45.52 +/- 7.49/microL for deletions of 3p22.1/CEP3. Numbers of CACs with deletions of 3p22.1, 10q22.3, and 9p21.3, and gains of URO, increased significantly from early to advanced stage of disease.
Conclusions: We have developed a sensitive and quantitative antigen-independent FISH-based test for detecting CACs in peripheral blood of patients with NSCLC, which showed a significant correlation with the presence of cancer. If this pilot study can be validated in a larger study, CACs may have a role in the management of patients with NSCLC.
(c) 2010 AACR.
Figures




Similar articles
-
Detection of circulating genetically abnormal cells using 4-color fluorescence in situ hybridization for the early detection of lung cancer.J Cancer Res Clin Oncol. 2021 Aug;147(8):2397-2405. doi: 10.1007/s00432-021-03517-6. Epub 2021 Feb 6. J Cancer Res Clin Oncol. 2021. PMID: 33547948 Free PMC article.
-
3p22.1 and 10q22.3 deletions detected by fluorescence in situ hybridization (FISH): a potential new tool for early detection of non-small cell lung Cancer (NSCLC).J Thorac Oncol. 2008 Sep;3(9):979-84. doi: 10.1097/JTO.0b013e3181834f3a. J Thorac Oncol. 2008. PMID: 18758299 Free PMC article.
-
Comparison of molecular abnormalities in bronchial brushings and tumor touch preparations.Cancer. 2005 Feb 25;105(1):35-43. doi: 10.1002/cncr.20800. Cancer. 2005. PMID: 15605362
-
[Research progress of circulating tumor DNA methylation in non-small cell lung cancer].Zhonghua Jie He He Hu Xi Za Zhi. 2018 Dec 12;41(12):967-970. doi: 10.3760/cma.j.issn.1001-0939.2018.12.013. Zhonghua Jie He He Hu Xi Za Zhi. 2018. PMID: 30522195 Review. Chinese. No abstract available.
-
Identification of differentially expressed circulating serum microRNA for the diagnosis and prognosis of Indian non-small cell lung cancer patients.Curr Probl Cancer. 2020 Aug;44(4):100540. doi: 10.1016/j.currproblcancer.2020.100540. Epub 2020 Jan 23. Curr Probl Cancer. 2020. PMID: 32007320 Review.
Cited by
-
A Classifier for Improving Early Lung Cancer Diagnosis Incorporating Artificial Intelligence and Liquid Biopsy.Front Oncol. 2022 Mar 2;12:853801. doi: 10.3389/fonc.2022.853801. eCollection 2022. Front Oncol. 2022. PMID: 35311112 Free PMC article.
-
Molecular profiling of individual tumor cells by hyperspectral microscopic imaging.Transl Res. 2012 May;159(5):366-75. doi: 10.1016/j.trsl.2011.08.003. Epub 2011 Sep 3. Transl Res. 2012. PMID: 22500509 Free PMC article.
-
The identification and characterization of breast cancer CTCs competent for brain metastasis.Sci Transl Med. 2013 Apr 10;5(180):180ra48. doi: 10.1126/scitranslmed.3005109. Sci Transl Med. 2013. PMID: 23576814 Free PMC article.
-
Application of circulating genetically abnormal cells in the diagnosis of early-stage lung cancer.J Cancer Res Clin Oncol. 2022 Mar;148(3):685-695. doi: 10.1007/s00432-021-03648-w. Epub 2021 Apr 24. J Cancer Res Clin Oncol. 2022. PMID: 33893839 Free PMC article.
-
On the origin and destination of cancer stem cells: a conceptual evaluation.Am J Cancer Res. 2013;3(1):107-16. Epub 2013 Jan 18. Am J Cancer Res. 2013. PMID: 23359140 Free PMC article.
References
-
- Fehm T, Sagalowsky A, Beitsch P, et al. Cytogenetic evidence that circulating epithelial cells in patients with carcinoma are malignant. Clinical Cancer Research. 2002 July;8:2073–2084. - PubMed
-
- Cristofanilli M, Budd GT, Ellis MJ, et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med. 2004;351:781–791. - PubMed
-
- Hayes DF, Cristofanilli M, Budd GT, et al. Circulating tumor cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin Cancer Res. 2006;12:4218–4224. - PubMed
-
- De Bono JS, Scher HI, Montgomery RB, et al. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res. 2008;14:6302–6309. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
