

Ovarian cancer development and metastasis
- PMID: 20651229
- PMCID: PMC2928939
- DOI: 10.2353/ajpath.2010.100105
Ovarian cancer development and metastasis
Abstract
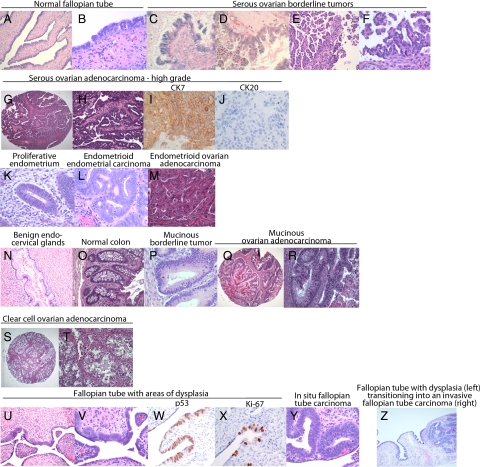
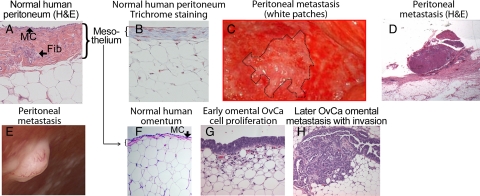
The biology of ovarian carcinoma differs from that of hematogenously metastasizing tumors because ovarian cancer cells primarily disseminate within the peritoneal cavity and are only superficially invasive. However, since the rapidly proliferating tumors compress visceral organs and are only temporarily chemosensitive, ovarian carcinoma is a deadly disease, with a cure rate of only 30%. There are a number of genetic and epigenetic changes that lead to ovarian carcinoma cell transformation. Ovarian carcinoma could originate from any of three potential sites: the surfaces of the ovary, the fallopian tube, or the mesothelium-lined peritoneal cavity. Ovarian cacinoma tumorigenesis then either progresses along a stepwise mutation process from a slow growing borderline tumor to a well-differentiated carcinoma (type I) or involves a genetically unstable high-grade serous carcinoma that metastasizes rapidly (type II). During initial tumorigenesis, ovarian carcinoma cells undergo an epithelial-to-mesenchymal transition, which involves a change in cadherin and integrin expression and up-regulation of proteolytic pathways. Carried by the peritoneal fluid, cancer cell spheroids overcome anoikis and attach preferentially on the abdominal peritoneum or omentum, where the cancer cells revert to their epithelial phenotype. The initial steps of metastasis are regulated by a controlled interaction of adhesion receptors and proteases, and late metastasis is characterized by the oncogene-driven fast growth of tumor nodules on mesothelium covered surfaces, causing ascites, bowel obstruction, and tumor cachexia.
Figures
Comment in
-
Ovarian tumors metastasize in blood.Cancer Discov. 2014 Sep;4(9):OF2. doi: 10.1158/2159-8290.CD-NB2014-116. Epub 2014 Jul 31. Cancer Discov. 2014. PMID: 25185201
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, Thun M. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Eisenkop S, Spirtos NM. The clinical significance of occult macroscopically positive retroperitoneal nodes in patients with epithelial ovarian cancer. Gynecol Oncol. 2001;82:143–149. - PubMed
-
- Bristow RE, del Carmen M, Kaufman H, Montz FJ. Radical oophorectomy with primary stapled colorectal anastomosis for resection of locally advanced epithelial ovarian cancer. J Am Coll Surg. 2003;197:565–574. - PubMed
-
- Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. 2002;20:1248–1259. - PubMed
-
- Winter WE, Maxwell L, Tian C, Carlson JW, Ozols RF, Rose P, Markmann M, Armstrong DK, Muggia F, McGuire WP. Prognostic factors for stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. J Clin Oncol. 2007;25:3621–3627. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
