

Vasomotor symptoms and coronary artery calcium in postmenopausal women
- PMID: 20651617
- PMCID: PMC3037019
- DOI: 10.1097/gme.0b013e3181e664dc
Vasomotor symptoms and coronary artery calcium in postmenopausal women
Abstract
Objective: We assessed whether vasomotor symptoms (VMS) are associated with coronary artery calcium (CAC) and how hormone therapy (HT) may influence this association.
Methods: Participants were a subset of women aged 50 to 59 years with a history of hysterectomy who were enrolled in the Women's Health Initiative (WHI) estrogen-alone clinical trial and underwent a CT scan of the chest at the end of the trial to determine CAC. Participants provided information about VMS (hot flashes and/or night sweats), as well as HT use, on self-administered questionnaires at trial baseline.
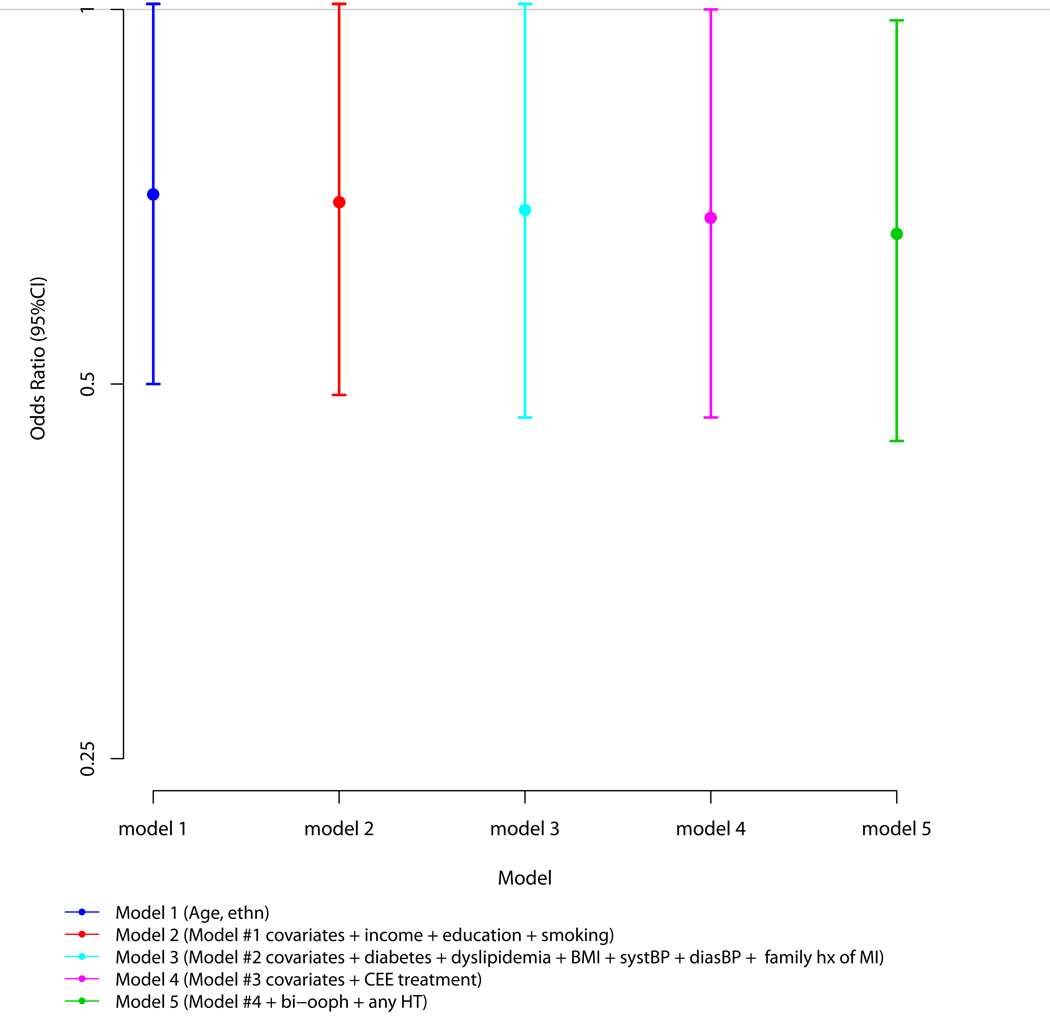
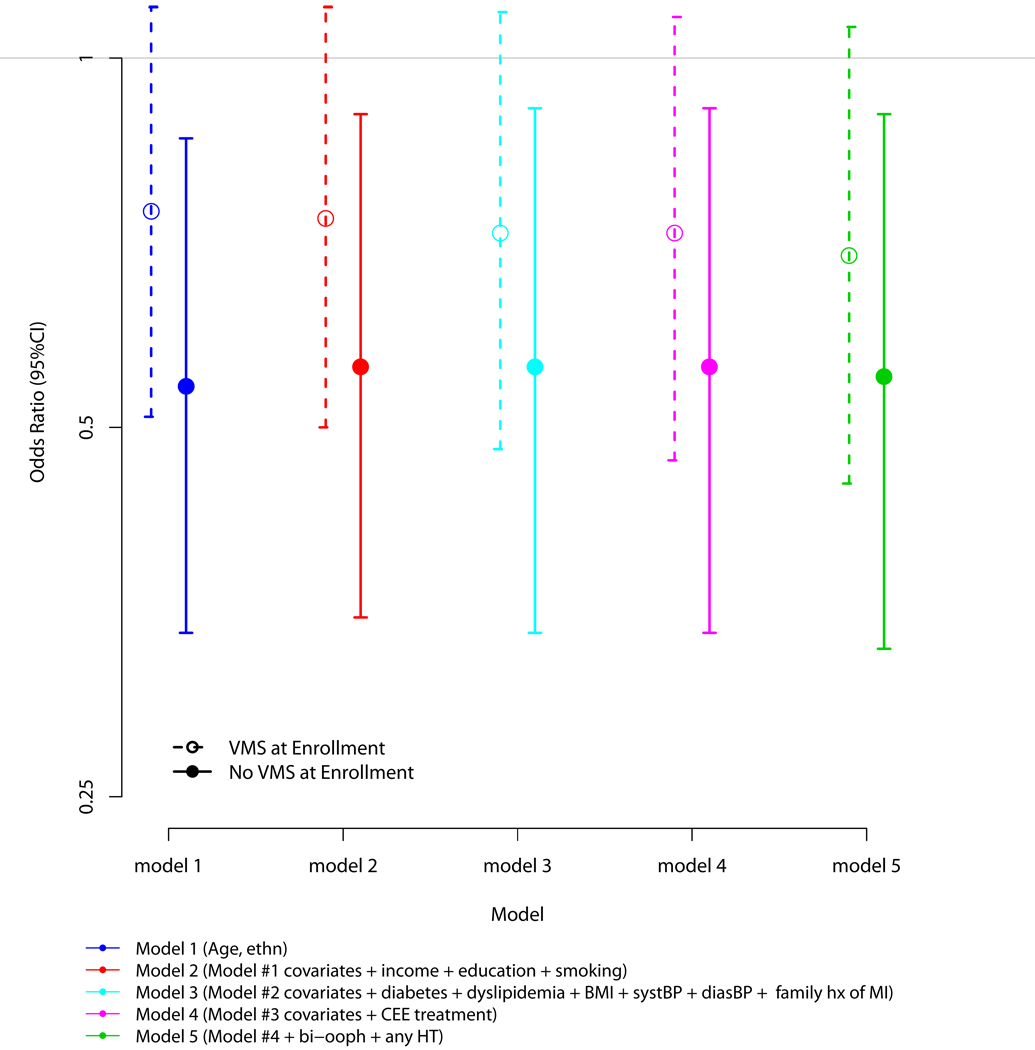
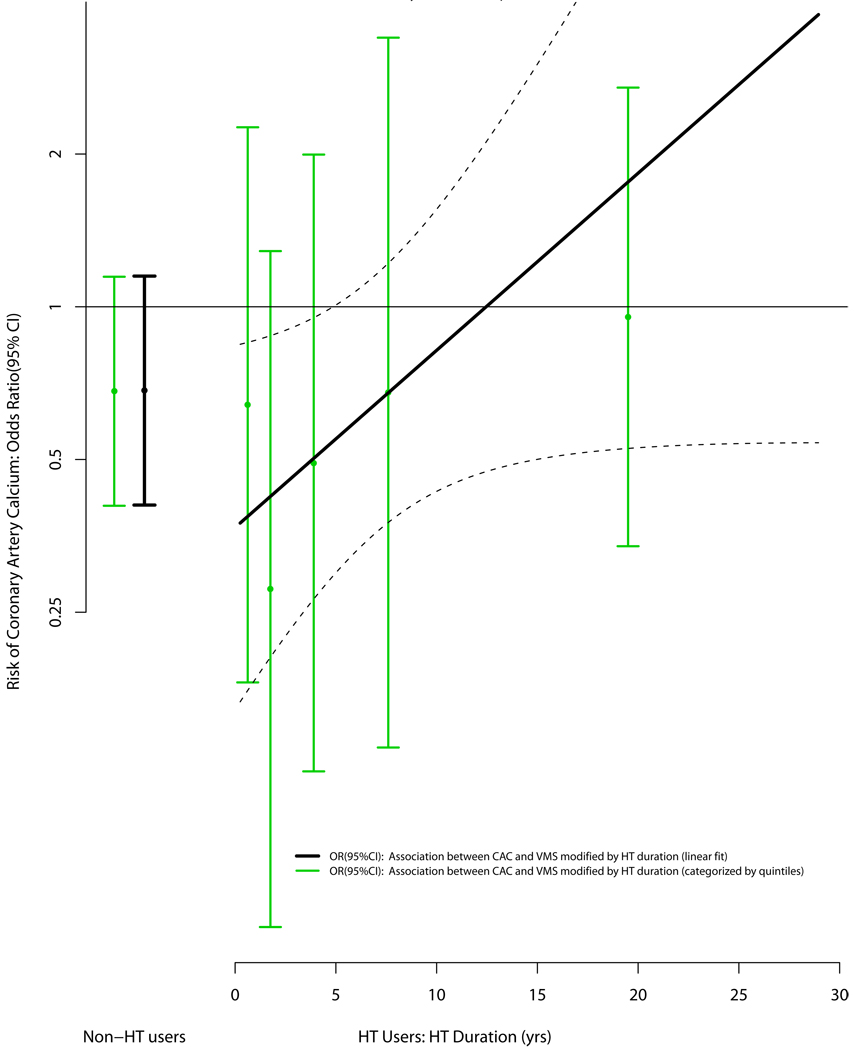
Results: The sample consisted of 918 women with a mean (SD) age of 55.1 (2.8) years at WHI randomization and 64.8 (2.9) years at CAC ascertainment. The prevalence of a CAC score higher than 0 was 46%, whereas the prevalence of a CAC score of 10 or higher and higher than 100 was 39% and 19%, respectively. At randomization, 77% reported a history of any VMS at any time before or at enrollment in the WHI, whereas 20% reported any VMS present only at enrollment. Compared with those without a history of any VMS and after adjustment for potential confounders, a history of any VMS at any time up to and including WHI enrollment was associated with significantly reduced odds for CAC higher than 0 (odds ratio, 0.66; 95% CI, 0.45-0.98). Moreover, as duration of HT increased, the inverse association between any VMS and CAC moved toward the null.
Conclusions: A history of any VMS was significantly associated with reduced odds for CAC independent of traditional cardiovascular disease risk factors and other relevant covariates. This association seems to be influenced by duration of HT.
Conflict of interest statement
None
Figures
Comment in
-
Flash of insight or flush of confusion?Menopause. 2010 Nov-Dec;17(6):1108-10. doi: 10.1097/gme.0b013e3181e851f9. Menopause. 2010. PMID: 20613667 No abstract available.
References
-
- Porter M, Penney GC, Russell D, Russell E, Templeton A. A population based survey of women's experience of the menopause. BJOG: An International Journal of Obstetrics & Gynaecology. 1996;103:1025–1028. - PubMed
-
- N. I. H. State-of-the-Science Panel. National Institutes of Health State-of-the-Science Conference Statement: Management of Menopause-Related Symptoms. Ann Intern Med. 2005;142:1003–1013. - PubMed
-
- Barnabei VM, Grady D, Stovall DW, et al. Menopausal Symptoms in Older Women and the Effects of Treatment With Hormone Therapy. Obstet Gynecol. 2002;100:1209–1218. - PubMed
-
- Simon J, Klaiber E, Wiita B, Bowen AH-MY. Differential Effects of Estrogen-Androgen and Estrogen-Only Therapy on Vasomotor Symptoms, Gonadotropin Secretion, and Endogenous Androgen Bioavailability in Postmenopausal Women. Menopause (New York, NY. 1999;6:138–146. - PubMed
-
- Guthrie JR, Dennerstein L, Hopper JL, Burger HG. Hot flushes, menstrual status, and hormone levels in a population-based sample of midlife women. Obstet Gynecol. 1996;88:437–442. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
