

An interactive teaching device simulating intussusception reduction
- PMID: 20652235
- PMCID: PMC2950270
- DOI: 10.1007/s00247-010-1764-x
An interactive teaching device simulating intussusception reduction
Abstract
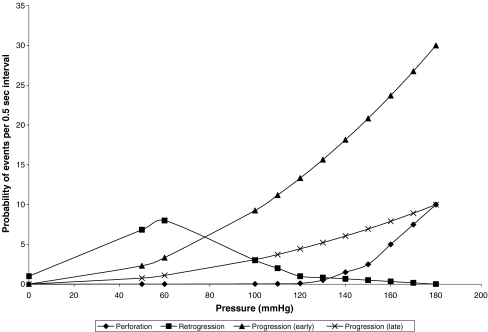
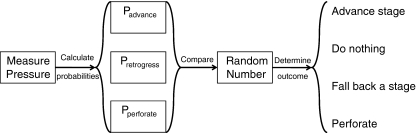
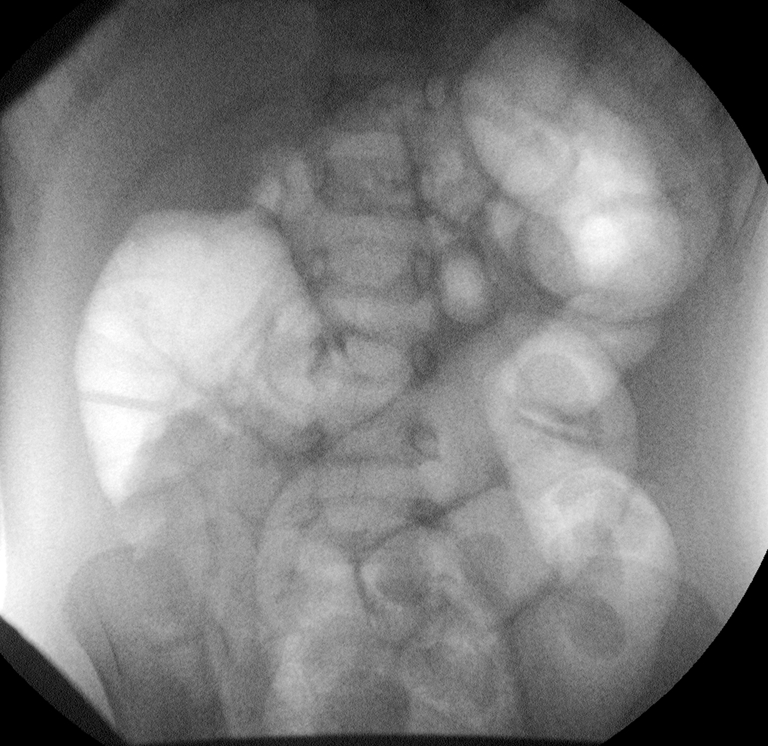
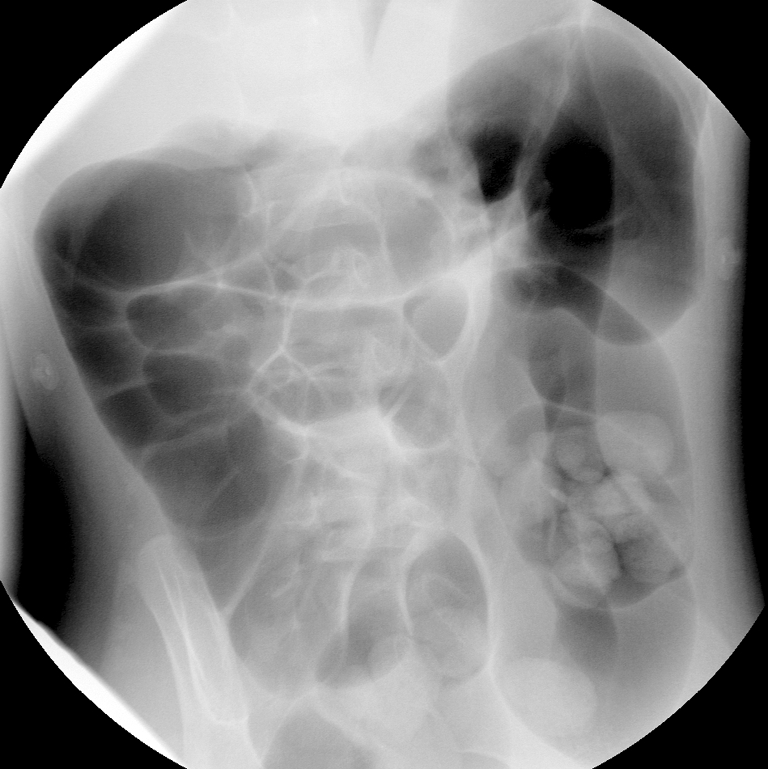
Intussusception is relatively uncommon, occurring in 0.5 to 2.3 cases per 1,000 live births in the USA. Radiology residents, therefore, have few opportunities to participate in intussusception reduction during training, and practicing radiologists encounter it infrequently. Training is essential, as successful reduction avoids surgery. The judgment involved in reducing an intussusception is best gained with experience. We developed a training device that simulates fluoroscopic intussusception reduction with air. The device consists of a doll that contains a cylinder with similar stress and strain characteristics to the human colon. The trainee pumps air into the cylinder through a rectal tube using a standard hand-held air reduction pump. A sensor measures the pressure within the chamber and transmits readings to a computer, which displays images from actual intussusception reductions based on the pressure maintained within the device. A random component in the software gives the user a new experience each time and models uncertainties in the actual reduction process, including perforation. This intussusception reduction simulator can enhance resident education, giving residents the opportunity to practice this technique before employing it on a real patient. The simulator can also help practicing radiologists become more comfortable with intussusception air reduction.
Figures



Similar articles
-
Radiology residents' experience with intussusception reduction.Pediatr Radiol. 2011 Jun;41(6):721-6. doi: 10.1007/s00247-010-1923-0. Epub 2010 Dec 22. Pediatr Radiol. 2011. PMID: 21174083 Free PMC article.
-
Simple device for air reduction of intussusception.Pediatr Radiol. 1990;20(6):472-4. doi: 10.1007/BF02075213. Pediatr Radiol. 1990. PMID: 2392367
-
Computer-based simulator for radiology: an educational tool.Radiographics. 2008 Jan-Feb;28(1):309-16. doi: 10.1148/rg.281075051. Radiographics. 2008. PMID: 18203945
-
Air intussusception reduction: "the winds of change".Pediatr Radiol. 1995;25(2):89-91. doi: 10.1007/BF02010312. Pediatr Radiol. 1995. PMID: 7596671 Review.
-
UK intussusception audit: a national survey of practice and audit of reduction rates.Clin Radiol. 2014 Apr;69(4):344-9. doi: 10.1016/j.crad.2013.10.024. Epub 2013 Dec 17. Clin Radiol. 2014. PMID: 24360511 Review.
Cited by
-
Unpacking the Broad Landscape of Intraoperative Stressors for Clinical Personnel: A Mixed-Methods Systematic Review.J Multidiscip Healthc. 2023 Jul 17;16:1953-1977. doi: 10.2147/JMDH.S401325. eCollection 2023. J Multidiscip Healthc. 2023. PMID: 37484819 Free PMC article. Review.
-
Air enema reduction of intussusception: a registrar-led, protocol-driven service is safe and effective.Pediatr Surg Int. 2013 Aug;29(8):805-9. doi: 10.1007/s00383-013-3328-2. Epub 2013 Jun 4. Pediatr Surg Int. 2013. PMID: 23732829
-
Upper gastrointestinal fluoroscopic simulator for neonates with bilious emesis.Pediatr Radiol. 2015 Aug;45(9):1413-6. doi: 10.1007/s00247-015-3330-z. Epub 2015 Mar 22. Pediatr Radiol. 2015. PMID: 25796384
-
Radiology residents' experience with intussusception reduction.Pediatr Radiol. 2011 Jun;41(6):721-6. doi: 10.1007/s00247-010-1923-0. Epub 2010 Dec 22. Pediatr Radiol. 2011. PMID: 21174083 Free PMC article.
-
Evaluation of a pediatric fluoroscopy training module to improve performance of upper gastrointestinal procedures in neonates with bilious emesis.Pediatr Radiol. 2016 Nov;46(12):1680-1683. doi: 10.1007/s00247-016-3674-z. Epub 2016 Aug 25. Pediatr Radiol. 2016. PMID: 27558686
References
-
- Swischuk LE, John SD, Swischuk PN. Spontaneous reduction of intussusception: verification with US. Radiology. 1994;192:269–271. - PubMed
-
- Meyer JS, Dangman BC, Buonomo C, et al. Air and liquid contrast agents in the management of intussusception: a controlled randomized trial. Radiology. 1993;188:507–511. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
