

Practice patterns for antibiotic de-escalation in culture-negative healthcare-associated pneumonia
- PMID: 20652354
- PMCID: PMC2945711
- DOI: 10.1007/s15010-010-0042-z
Practice patterns for antibiotic de-escalation in culture-negative healthcare-associated pneumonia
Abstract
Background: Published guidelines for the treatment of healthcare-associated pneumonia (HCAP) recommend initial broad-spectrum antibiotics with appropriate de-escalation based on culture results. Guideline recommendations are based on data from intubated patients, in whom cultures are easily obtained. The approach to antibiotic de-escalation for culture-negative patients has not been addressed. Consequently, there are no published reports that describe the current standard of practice.
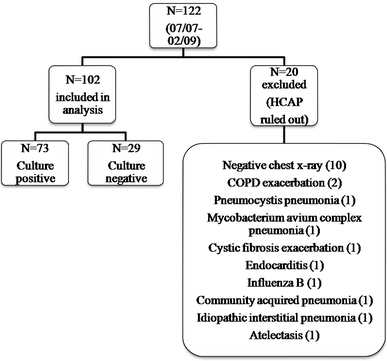
Patients and methods: All patients admitted to a university hospital with a diagnosis of HCAP, as defined by use of a pneumonia orderset, were identified retrospectively over a 2-year period. Antibiotics prescribed on admission, during hospital stay, and on discharge were recorded. De-escalation was defined as a change in the initial antibiotic therapy from broad- to narrow-spectrum coverage within 14 days of the initial prescription. The Pneumonia Severity Index was used for risk-adjustment.
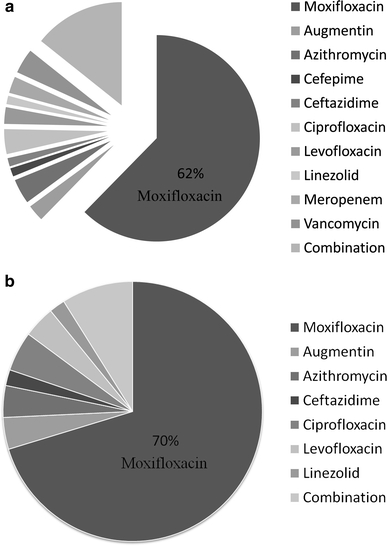
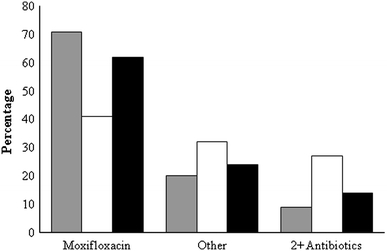
Results: A total of 102 patients were included in the analysis; of these, 72% (n = 73) were culture-negative. There were more males in the culture-negative than culture-positive group; otherwise, baseline characteristics were similar. Antibiotic therapy was de-escalated in 75% of the culture-negative group and 77% of the culture-positive group (p = 1.00). Culture-negative patients were de-escalated approximately 1 day earlier than culture-positive patients (3.93 vs. 5.04 days, p = 0.03). Culture-negative patients who were de-escalated had a shorter length of hospitalization, lower hospital costs, and lower mortality rates. In 70% of the culture-negative patients, a respiratory fluoroquinolone was chosen for de-escalation.
Conclusion: In this single-center study, most of the patients with culture-negative HCAP were safely de-escalated to a respiratory fluoroquinolone.
Figures
References
-
- Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416. - PubMed
-
- Venditti M, Falcone M, Corrao S, et al. Outcomes of patients hospitalized with community-acquired, health care-associated, and hospital-acquired pneumonia. Ann Intern Med. 2009;150:19–26. - PubMed
