

Virtual liver resection and volumetric analysis of the future liver remnant using open source image processing software
- PMID: 20652701
- PMCID: PMC2936678
- DOI: 10.1007/s00268-010-0663-5
Virtual liver resection and volumetric analysis of the future liver remnant using open source image processing software
Abstract
Background: After extended liver resection, a remnant liver that is too small can lead to postresection liver failure. To reduce this risk, preoperative evaluation of the future liver remnant volume (FLRV) is critical. The open-source OsiriX PAC software system can be downloaded for free and used by nonradiologists to calculate liver volume using a stand-alone Apple computer. The purpose of this study was to assess the accuracy of OsiriX CT volumetry for predicting liver resection volume and FLVR in patients undergoing partial hepatectomy.
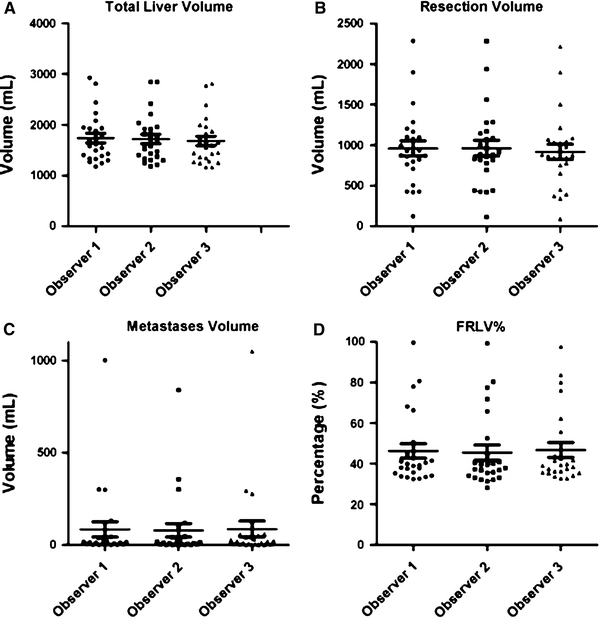
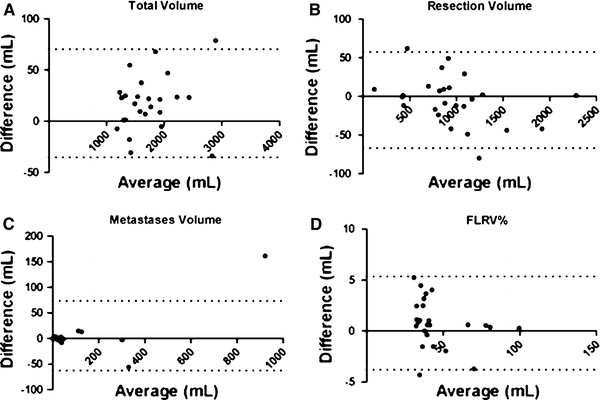
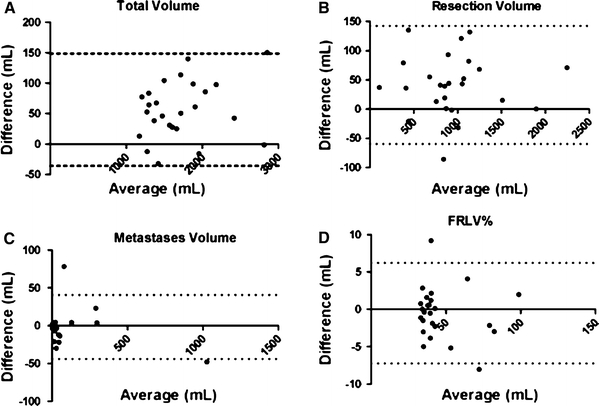
Methods: Preoperative contrast-enhanced liver CT scans of patients who underwent partial hepatectomy were analyzed by three observers. Two surgical trainees measured the total liver volume, resection volume, and tumor volume using OsiriX, and a radiologist measured these volumes using CT scanner-linked Aquarius iNtuition software. Resection volume was correlated with prospectively determined resection weight, and differences in the measured liver volumes were analyzed. Interobserver variability was assessed using Bland-Altman plots.
Results: 25 patients (M/F ratio: 13/12) with a median age of 61 (range, 34-77) years were included. There were significant correlations between the weight and volume of the resected specimens (Pearson's correlation coefficient: R(2) = 0.95). There were no major differences in total liver volumes, resection volumes, or tumor volumes for observers 1, 2, and 3. Bland-Altman plots showed a small interobserver variability. The mean time to complete liver volumetry for one patient using OsiriX was 19 +/- 3 min.
Conclusions: OsiriX liver volumetry performed by surgeons is an accurate and time-efficient method for predicting resection volume and FLRV.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
