

Vancomycin dosing assessment in intensive care unit patients based on a population pharmacokinetic/pharmacodynamic simulation
- PMID: 20653673
- PMCID: PMC2911550
- DOI: 10.1111/j.1365-2125.2010.03679.x
Vancomycin dosing assessment in intensive care unit patients based on a population pharmacokinetic/pharmacodynamic simulation
Abstract
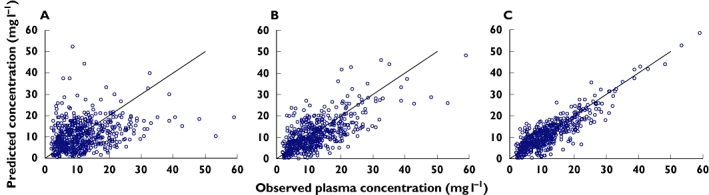
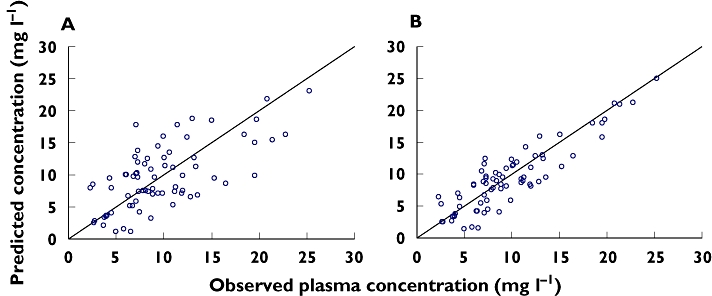
WHAT IS ALREADY KNOWN ABOUT THIS SUBJECT * Despite the frequent use of vancomycin in intensive care unit (ICU) patients, few studies aimed at characterizing vancomycin population pharmacokinetics have been performed in this critical population. * Population pharmacokinetics coupled with pharmacodynamic analysis, in order to optimize drug exposure and hence antibacterial effectiveness, has been little applied in these specific patients. WHAT THIS STUDY ADDS * Our population model characterized the pharmacokinetic profile of vancomycin in adult ICU patients, higher distribution volume values (V) being observed when the patient's serum creatinine (Cr(Se)) was greater than 1 mg dl(-1). * Age and creatinine clearance (CL(cr)) were identified as the main covariates explaining the pharmacokinetic variability in vancomycin CL. * Our pharmacokinetic/pharmacodynamic (PK/PD) simulation should aid clinicians to select initial vancomycin doses that will maximize the rate of response in the ICU setting, taking into account the patient's age and renal function as well as the susceptibility of Staphylococcus aureus. AIM To estimate the vancomycin pharmacokinetic profile in adult ICU patients and to assess vancomycin dosages for increasing the likelihood of optimal exposure. METHODS Five hundred and sixty-nine concentration-time data from 191 patients were analysed using a population pharmacokinetic approach (NONMEN). External model evaluation was made in 46 additional patients. The 24 h area under the concentration-time curve (AUC(0,24 h)) was derived from the final model. Minimum inhibitory concentration (MIC) values for S. aureus were obtained from the EUCAST database. AUC(0,24 h) : MIC >/= 400 was considered as PK/PD efficacy index. The probability of different dosages attaining the target considering different strains of S. aureus and patient subgroups was estimated with Monte Carlo simulation. RESULTS Vancomycin CL showed a significant dependence on patient age and renal function whereas Cr(Se) > 1 mg dl(-1) increased V more than twofold. For our representative ICU patient, 61 years, 73 kg, Cr(Se)= 1.4 mg dl(-1), measured CL(Cr)= 74.7 ml min(-1), the estimated values were CL = 1.06 ml min(-1) kg(-1) and V= 2.04 l kg(-1). The cumulative fraction of response for a standard vancomycin dose (2 g day(-1)) was less than 25% for VISA strains, and 33% to 95% for susceptible S. aureus, depending on patient characteristics. CONCLUSIONS Simulations provide useful information regarding the initial assessment of vancomycin dosing, the conventional dosing regimen probably being suboptimal in adult ICU patients. A graphic approach provides the recommended dose for any selected probability of attaining the PK/PD efficacy target or to evaluate the cumulative fraction of response for any dosing regimen in this population.
Figures
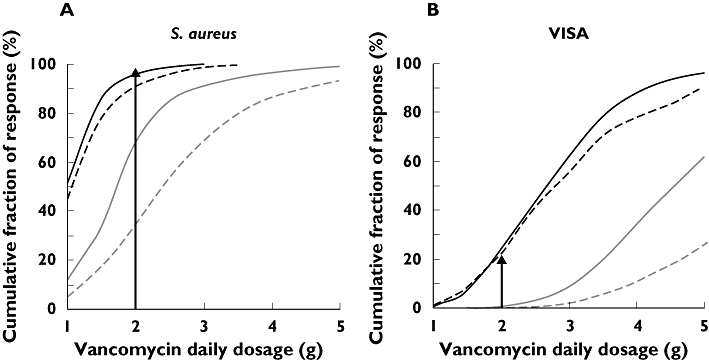
 ); CLCr≤ 60 ml min−1 and Age ≤ 65 years (
); CLCr≤ 60 ml min−1 and Age ≤ 65 years ( ); CLCr > 60 ml min−1 and Age > 65 years (
); CLCr > 60 ml min−1 and Age > 65 years ( ); CLCr > 60 ml min−1 and Age ≤ 65 years (
); CLCr > 60 ml min−1 and Age ≤ 65 years ( )
)References
-
- Klevens RM, Edwards JR, Tenover FC, McDonald LC, Horan T, Gaynes R. Changes in the epidemiology of methicillin-resistant Staphylococcus aureus in intensive care units in US hospitals, 1992–2003. Clin Infect Dis. 2006;42:389–91. - PubMed
-
- Alvarez-Lerma F. Modification of empiric antibiotic treatment in patients with pneumonia acquired in the intensive care unit. ICU-Acquired Pneumonia Study Group. Intensive Care Med. 1996;22:387–94. - PubMed
-
- Rello J, Gallego M, Mariscal D, Sonora R, Valles J. The value of routine microbial investigation in ventilator-associated pneumonia. Am J Respir Crit Care Med. 1997;156:196–200. - PubMed
-
- Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef MH. The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting. Chest. 2000;118:146–55. - PubMed
-
- Kollef MH. Improving outcomes in the ICU setting: are we effectively using all of the information that is potentially available to us? Chest. 1999;115:1490–2. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
