

Long-term survivors of childhood Ewing sarcoma: report from the childhood cancer survivor study
- PMID: 20656964
- PMCID: PMC2948841
- DOI: 10.1093/jnci/djq278
Long-term survivors of childhood Ewing sarcoma: report from the childhood cancer survivor study
Abstract
Background: The survival of Ewing sarcoma (ES) patients has improved since the 1970s but is associated with considerable future health risks.
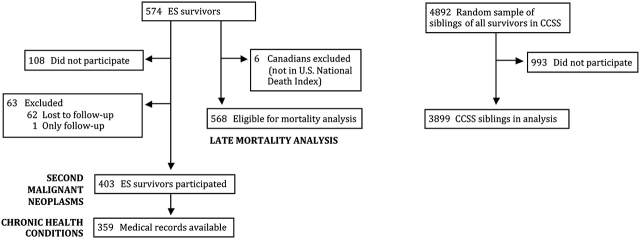
Methods: The study population consisted of long-term (> or =5-year) survivors of childhood ES diagnosed before age 21 from 1970 to 1986. Cause-specific mortality was evaluated in eligible survivors (n = 568), and subsequent malignant neoplasms, chronic health conditions, infertility, and health status were evaluated in the subset participating in the Childhood Cancer Survivor Study (n = 403). Outcomes were compared with the US population and sibling control subjects (n = 3899). Logistic, Poisson, or Cox proportional hazards models, with adjustments for sex, age, race/ethnicity, and potential intrafamily correlation, were used. Statistical tests were two-sided.
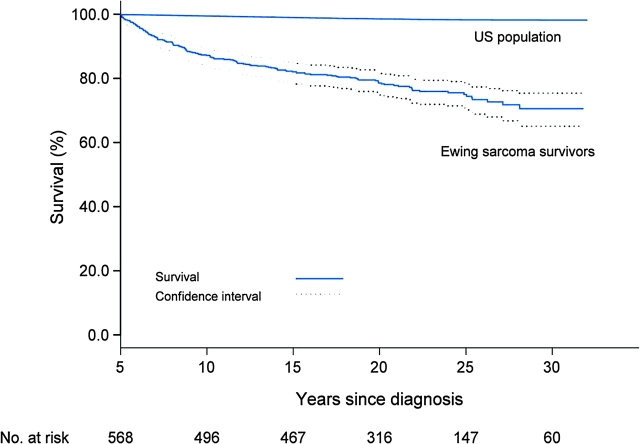
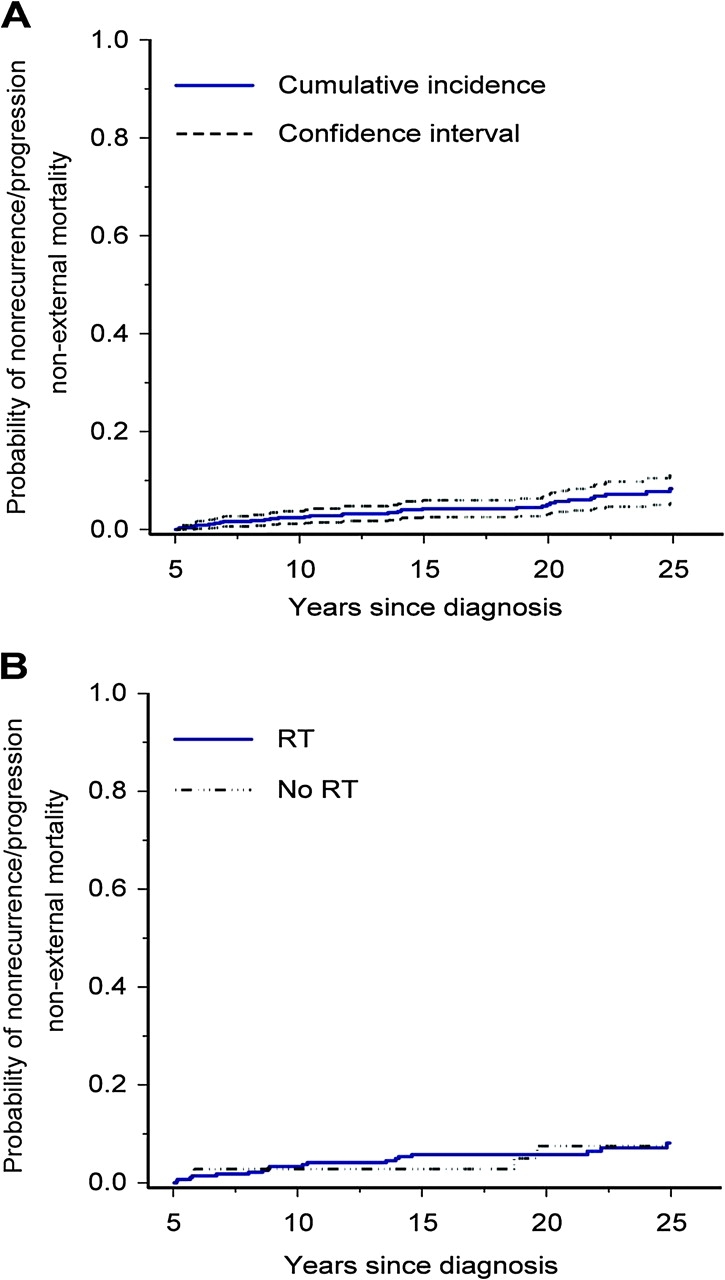
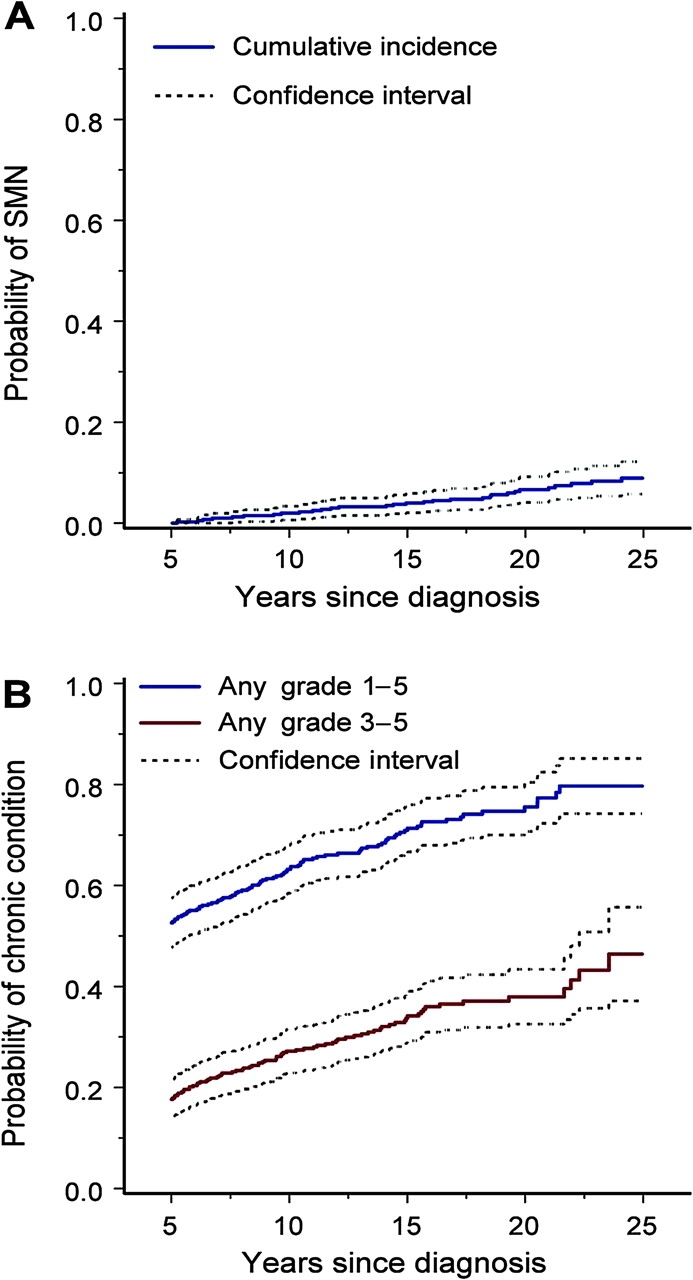
Results: Cumulative mortality of ES survivors was 25.0% (95% confidence interval [CI] = 21.1 to 28.9) 25 years after diagnosis. The all-cause standardized mortality ratio was 13.3 (95% CI = 11.2 to 15.8) overall, 23.1 (95% CI = 17.6 to 29.7) for women, and 10.0 (95% CI = 7.9 to 12.5) for men. The nonrecurrence-progression non-external cause standardized mortality ratio (subsequent non-ES malignant neoplasms and cardiac and pulmonary causes potentially attributable to ES treatment) was 8.7 (95% CI = 6.2 to 12.0). Twenty-five years after ES diagnosis, cumulative incidence of subsequent malignant neoplasms, excluding nonmelanoma skin cancers, was 9.0% (95% CI = 5.8 to 12.2). Compared with siblings, survivors had an increased risk of severe, life-threatening, or disabling chronic health conditions (relative risk = 6.0, 95% CI = 4.1 to 9.0). Survivors had lower fertility rates (women: P = .005; men: P < .001) and higher rates of moderate to extreme adverse health status (P < .001).
Conclusion: Long-term survivors of childhood ES exhibit excess mortality and morbidity.
Figures
References
-
- Bernstein M, Kovar H, Paulussen M, et al. Ewing sarcoma family of tumors: Ewing sarcoma of bone and soft tissue and the peripheral primitive neuroectodermal tumors. In: Pizzo P, Poplack D, editors. Principles and Practice of Pediatric Oncology. 5th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2005. pp. 1002–1032.
-
- Esiashvili N, Goodman M, Marcus RB., Jr Changes in incidence and survival of Ewing sarcoma patients over the past 3 decades: SEER data. J Pediatr Hematol Oncol. 2008;30(6):425–430. - PubMed
-
- Fuchs B, Valenzuela RG, Inwards C, Sim FH, Rock MG. Complications in long-term survivors of Ewing sarcoma. Cancer. 2003;98(12):2687–2692. - PubMed
-
- Mansky P, Arai A, Stratton P, et al. Treatment late effects in long-term survivors of pediatric sarcoma. Pediatr Blood Cancer. 2007;48(2):192–199. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
