

Minimally invasive versus open transforaminal lumbar interbody fusion
- PMID: 20657693
- PMCID: PMC2908364
- DOI: 10.4103/2152-7806.63905
Minimally invasive versus open transforaminal lumbar interbody fusion
Abstract
Background: Available clinical data are insufficient for comparing minimally invasive (MI) and open approaches for transforaminal lumbar interbody fusion (TLIF). To date, a paucity of literature exists directly comparing minimally invasive (MI) and open approaches for transforaminal lumbar interbody fusion (TLIF). The purpose of this study was to directly compare safety and effectiveness for these two surgical approaches.
Materials and methods: Open or minimally invasive TLIF was performed in 63 and 76 patients, respectively. All consecutive minimally invasive TLIF cases were matched with a comparable cohort of open TLIF cases using three variables: diagnosis, number of spinal levels, and history of previous lumbar surgery. Patients were treated for painful degenerative disc disease with or without disc herniation, spondylolisthesis, and/or stenosis at one or two spinal levels. Clinical outcome (self-report measures, e.g., visual analog scale (VAS), patient satisfaction, and MacNab's criteria), operative data (operative time, estimated blood loss), length of hospitalization, and complications were assessed. Average follow-up for patients was 37.5 months.
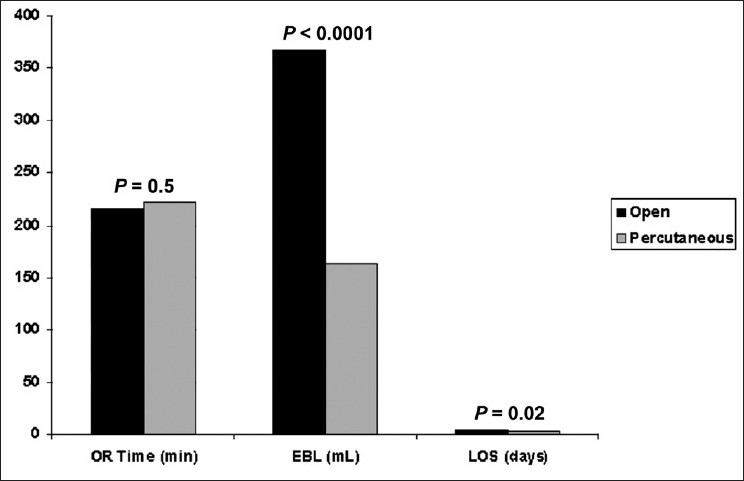
Results: The mean change in VAS scores postoperatively was greater (5.2 vs. 4.1) in theopen TLIF patient group (P = 0.3). MacNab's criteria score was excellent/good in 67% and 70% (P = 0.8) of patients in open and minimally invasive TLIF groups, respectively. The overall patient satisfaction was 72.1% and 64.5% (P = 0.4) in open and minimally invasive TLIF groups, respectively. The total mean operative time was 214.9 min for open and 222.5 min for minimally invasive TLIF procedures (P = 0.5). The mean estimated blood loss for minimally invasive TLIF (163.0 ml) was significantly lower (P < 0.0001) than the open approach (366.8 ml). The mean duration of hospitalization in the minimally invasive TLIF (3 days) was significantly shorter (P = 0.02) than the open group (4.2 days). The total rate of neurological deficit was 10.5% in the minimally invasive TLIF group compared to 1.6% in the open group (P = 0.02).
Conclusions: Minimally invasive TLIF technique may provide equivalent long-term clinical outcomes compared to open TLIF approach in select population of patients. The potential benefit of minimized tissue disruption, reduced blood loss, and length of hospitalization must be weighted against the increased rate of neural injury-related complications associated with a learning curve.
Keywords: Clinical outcomes; Complications; Degenerative lumbar spine; Lumbar fusion; Minimally invasive approach; Open approach; Transforaminal lumbar interbody fusion.
Figures
References
-
- Beringer WF, Mobasser JP. Unilateral pedicle screw instrumentation for minimally invasive transforaminal lumbar interbody fusion. Neurosurg Focus. 2006;20:E4. - PubMed
-
- Blume HG, Rojas CH. Unilateral lumbar interbody fusion (posterior approach) utilizing dowel graft. J Neurol Orthop Surg. 1981;2:171–5.
-
- Brislin B, Vaccaro AR. Advances in posterior lumbar interbody fusion. Orthop Clin North Am. 2002;33:367–74. - PubMed
-
- Coe JD. Instrumented transforaminal lumbar interbody fusion with bioabsorbable polymer implants and iliac crest autograft. Neurosurg Focus. 2004;16:E11. - PubMed
-
- Datta G, Gnanalingham KK, Peterson D, Mendoza N, O'Neill K, Van Dellen J, et al. Back pain and disability after lumbar laminectomy: is there a relationship to muscle retraction? Neurosurgery. 2004;54:1413–20. - PubMed
LinkOut - more resources
Full Text Sources
