

Cardiopulmonary Exercise Testing in Patients with Chronic Heart Failure: Prognostic Comparison from Peak VO2 and VE/VCO2 Slope
- PMID: 20657715
- PMCID: PMC2908890
- DOI: 10.2174/1874192401004010127
Cardiopulmonary Exercise Testing in Patients with Chronic Heart Failure: Prognostic Comparison from Peak VO2 and VE/VCO2 Slope
Abstract
Background: Cardiopulmonary exercise testing with ventilatory expired gas analysis (CPET) has proven to be a valuable tool for assessing patients with chronic heart failure (CHF). The maximal oxygen uptake (peak V02) is used in risk stratification of patients with CHF. The minute ventilation-carbon dioxide production relationship (VE/VCO2 slope) has recently demonstrated prognostic significance in patients with CHF.
Methods: Between January 2006 and December 2007 we performed CPET in 184 pts (146 M, 38 F, mean age 59.8 +/- 12.9 years), with stable CHF (96 coronary artery disease, 88 dilated cardiomyopathy), in NYHA functional class II (n.107) - III (n.77), with left ventricular ejection fraction (LVEF) </= 45%,. The ability of peak VO2 and VE/VCO2 slope to predict cardiac related mortality and cardiac related hospitalization within 12 months after evaluation was examined.
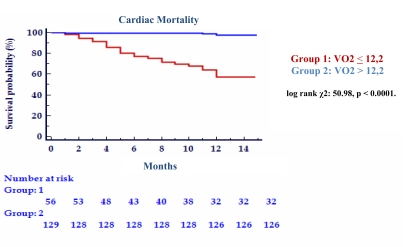
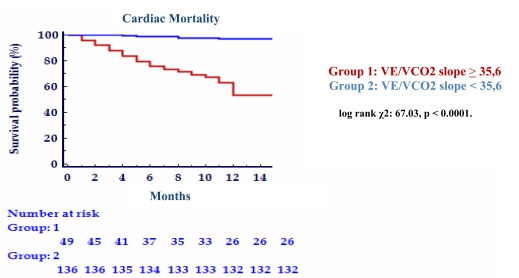
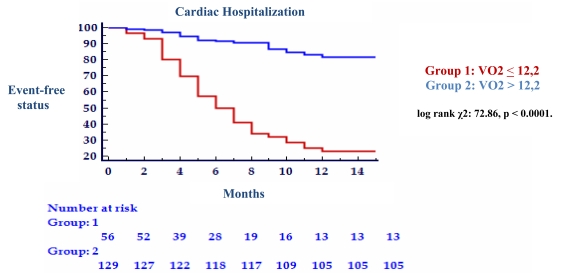
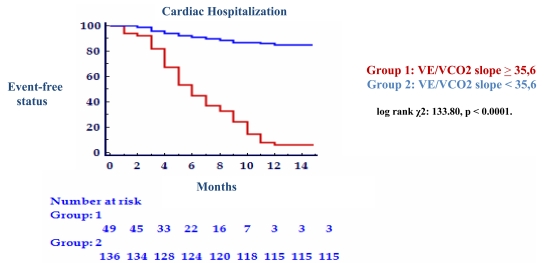
Results: Peak VO2 and VE/VCO2 slope were demonstrated with univariate Cox regression analysis both to be significant predictor of cardiac-related mortality and hospitalization (p < 0.0001, respectively). Non survivors had a lower peak VO2 (10.49 +/- 1.70 ml/kg/min vs. 14.41 +/- 3.02 ml/kg/min, p < 0.0001), and steeper Ve/VCO2 slope (41.80 +/- 8.07 vs. 29.84 +/- 6.47, p < 0.0001) than survivors. Multivariate survival analysis revealed that VE/VCO2 slope added additional value to VO2 peak as an independent prognostic factor (chi2: 56.48, relative risk: 1.08, 95% CI: 1.03 - 1.13, p = 0.001). The results from Kaplan-Meier analysis revealed a 1-year cardiac-related mortality of 75% in patients with VE/VCO2 slope >/= 35.6 and 25% in those with VE/VCO2 slope < 35.6 (log rank chi2: 67.03, p < 0.0001) and 66% in patients with peak VO2 </= 12.2 ml/kg/min and 34% in those with peak VO2 > 12.2 ml/kg/min (log rank chi2: 50.98, p < 0.0001). One-year cardiac-related hospitalization was 77% in patients with VE/VCO2 slope >/= 32.5 and 23% in those with VE/VCO2 slope < 32.5 (log rank chi2: 133.80, p < 0.0001) and 63% in patients with peak VO2 </= 12.3 ml/kg/min and 37% in those with peak VO2 > 12.3 ml/kg/min (log rank chi2: 72.86, p < 0.0001). The VE/VCO2 slope was demonstrated with receiver operating characteristic curve analysis to be equivalent to peak VO2 in predicting cardiac-related mortality (0.89 vs. 0.89). Although area under the receiver operating characteristic curve for the VE/VCO2 slope was greater than peak VO2 in predicting cardiac-related hospitalization (0.88 vs 0.82), the difference was no statistically significant (p = 0.13).
Conclusion: These results add to the present body of knowledge supporting the use of CPET in CHF patients. The VE/VCO2 slope, as an index of ventilatory response to exercise, is an excellent prognostic parameter and improves the risk stratification of CHF patients. It is easier to obtain than parameters of maximal exercise capacity and is of equivalent prognostic importance than peak VO2.
Keywords: Congestive heart failure; exercise capacity; gas exchange; prognosis.; ventilation.
Figures
References
-
- Cohn JN, Fowler MB, Bristow MR, et al. Safety and efficacy of carvedilol in severe heart failure. The US Carvedilol Heart Failure Study Group. J Card Fail J. 1997;3:173–9. - PubMed
-
- Parker M, Colucci WS, Sackner-Bernstein JD, et al. Double-blind, placebo-controlled study of the effects of carvedilol in patients with moderates to severe heart failure the PRECISE Trial: Prospective Randomized Evaluation of Carvedilol on Symptoms and Exercise. Circulation. 1996;94:2793–9. - PubMed
-
- Packer M, Bristow MR, Cohn JN, et al. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure: US Carvedilol Heart Failure Study Group. N Engl J Med. 1996;334:1349–55. - PubMed
-
- Pamboukian SV, Aminbakhsh A, Thompson CR, et al. l carvedilol improves functional class in patients with severe left ventricular dysfunction referred for heart transplantation. Clin Transplant. 1999;13:426–31. - PubMed
-
- Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH, Jr, Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation. 1991;83:778–86. - PubMed
LinkOut - more resources
Full Text Sources