

doi: 10.1016/j.yjmcc.2010.07.012.
Epub 2010 Jul 24.
The pathophysiological mechanism underlying Brugada syndrome: depolarization versus repolarization
Affiliations
- PMID: 20659475
- PMCID: PMC2932806
- DOI: 10.1016/j.yjmcc.2010.07.012
Item in Clipboard
The pathophysiological mechanism underlying Brugada syndrome: depolarization versus repolarization
J Mol Cell Cardiol.
2010 Oct.
Abstract
This Point/Counterpoint presents a scholarly debate of the mechanisms underlying the electrocardiographic and arrhythmic manifestations of Brugada syndrome (BrS), exploring in detail the available evidence in support of the repolarization vs. depolarization hypothesis.
Copyright 2010 Elsevier Ltd. All rights reserved.
Figures

Qualitative model of the depolarization hypothesis for the Type-1 Brugada syndrome ECG. For explanation, see text. Modified from Ref. [8] with permission.
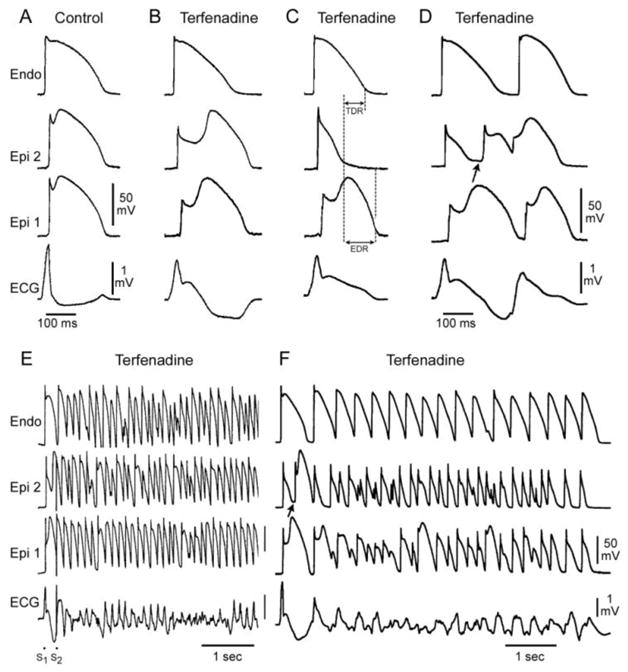
Cellular basis for electrocardiographic and arrhythmic manifestation of BrS. Each panel shows transmembrane action potentials from one endocardial (top) and two epicardial sites together with a transmural ECG recorded from a canine coronary-perfused right ventricular wedge preparation. A: Control (Basic cycle length (BCL) 400 msec). B: Combined sodium and calcium channel block with terfenadine (5 μM) accentuates the epicardial action potential notch creating a transmural voltage gradient that manifests as a ST segment elevation or exaggerated J wave in the ECG. Despite the appearance of a typical BrS ECG, an arrhythmogenic substrate is absent. C: Continued exposure to sodium and calcium blockade results in all-or-none repolarization at the end of phase 1 at some epicardial sites but not others, creating a local epicardial dispersion of repolarization (EDR) as well as a transmural dispersion of repolarization (TDR). D: Phase 2 reentry occurs when the epicardial action potential dome propagates from a site where it is maintained to regions where it has been lost giving rise to a closely coupled extrasystole. E: Extrastimulus (S1–S2 = 250 msec) applied to epicardium triggers a polymorphic VT. F: Phase 2 reentrant extrasystole triggers a brief episode of polymorphic VT. (Modified from [48] with permission)
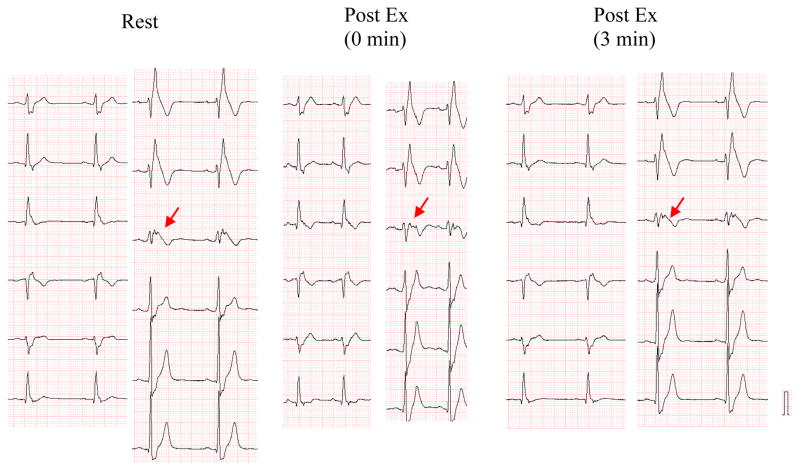
Opposite effects of exercise on QRS fragmentation and ST segment elevation in right precordial leads of a 33 year old asymptomatic male with Brugada syndrome secondary to a loss of function SCN5A missense mutation (R878C).
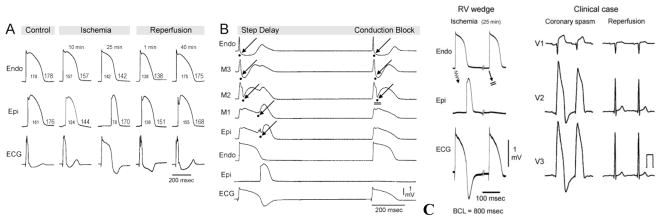
Electrophysiologic effect of ischemia in the ventricular wedge model. A: Each panel shows (from top to bottom) simultaneous recordings of transmembrane action potentials from endocardium (Endo) and epicardium (Epi) and the ECG recorded across the bath along the same axis. Recordings were obtained from a RV wedge displaying a relatively small phase 1 in the epicardial action potential under control conditions, following 10 and 25 min of no-flow ischemia, and 1 and 40 min of reperfusion. Progressive ischemia-induced delay of transmural conduction leads to a gradual prolongation of the R wave (apparent ST-segment elevation) and inversion of the T wave. B: Recordings obtained at 25–30 min of no-flow ischemia (BCL=800 msec). From top to bottom: Five unipolar electrograms (EGs) recorded between endocardium and epicardium (Endo, M3, M2, M1 and Epi), Endo action potential, Epi action potential and a transmural electrocardiogram (ECG). A 90 msec-step delay (discontinuous conduction) in transmural conduction occur between EG-M2 and EG-M1 giving rise to a prolonged R wave (tombstone morphology) and negative T wave in the ECG of alternate beats. 2:1 intramural conduction block occurs at site EG-M2 leads a disappearance of the ECG-T wave, which is concurrent with the absence of the Epi AP response. Arrows denote the activation time at each of the unipolar electrograms. C: Shown side-by side are recording from arterially-perfused right ventricular wedge preparation following 25–30 min of ischemia (BCL=800 msec)(Left) and an example of the tombstone effect and T wave alternans appearing in the right precordial leads following vasospastic ischemia as well as normalization of the ECG following spontaneous reperfusion. (Panels A, B and the left part of panel C are modified from [67] and right part of panel C is from Childers [69], with permission).
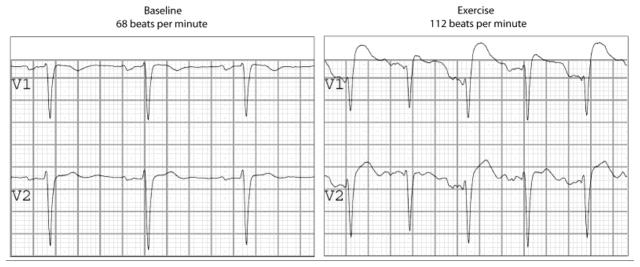
Exercise in a Brugada syndrome patient. It is clear that the tachycardia induced by exercise is accompanied by a sharp rise in ST-elevation and a coved-type morphology in V1, and, interestingly, alternating in this particular case. Courtesy of A.S. Amin, MD, and H.L. Tan, MD, PhD.
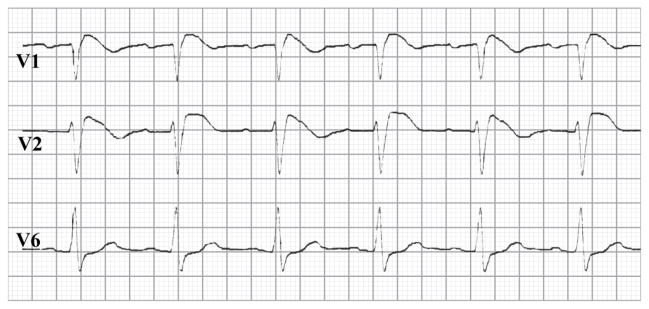
Alternating T-waves in a Brugada syndrome patient. Courtesy of H.L. Tan, MD, PhD.
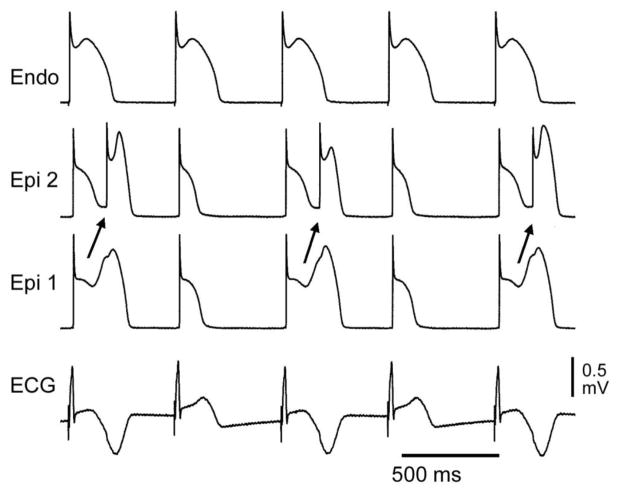
Appearance of T wave in alternate beats in an experitmental model of BrS generated by exposing a canine right ventricular wedge prpearation to verapamil (1 μM). T wave alternans occurs as a result of concealed phase 2 reentry. The dome propagates from Epi 1 to Epi 2 on alternating beats while the endocardial response remains constant. The concealed phase 2 reentry results in a negative T wave in alternate beats only. BCL=558 ms. Modified form [81], with permission.
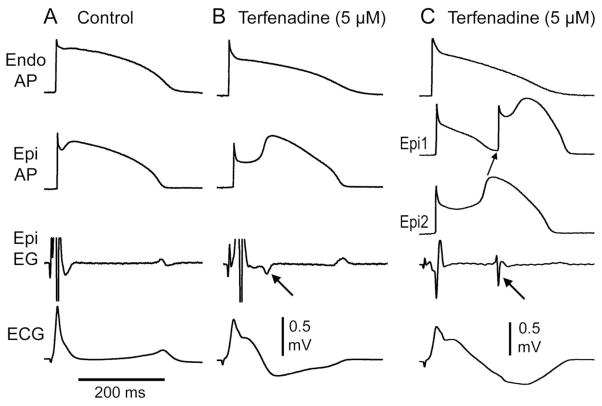
Late potentials due to the delayed second upstroke of the epicardial response or to concelaed phase 2 reentry generated in a canine right ventricular wedge model of Brugada sydnrome. A: Control. B: BrS phenotype develops following exposure to the INa and ICa inhibitor terfenadine (5 uM); a late potential is registered in the the epicardial electrogram following an 80 ms delay coincident with the upstroke of phase 2 of the action potential (arrow). C: Further exposure to terfenadine leads to loss of the action potnatil dome at some epicardial sites (Epi 1) but not others leading to the development of a concealed phase 2 reentry which regsiters in the epicardial electrogram as a late pottnial with a 148 ms delay (arrow). Modified form [82], with permission.
References
-
- Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol. 1992;20:1391–6. - PubMed
-
- Antzelevitch C, Brugada P, Borggrefe M, Brugada J, Brugada R, Corrado D, et al. Brugada syndrome: report of the second consensus conference. Heart Rhythm. 2005;2:429–40. - PubMed
-
- Eckardt L, Probst V, Smits JP, Bahr ES, Wolpert C, Schimpf R, et al. Long-term prognosis of individuals with right precordial ST-segment-elevation Brugada syndrome. Circulation. 2005;111:257–63. - PubMed
-
- Priori SG, Napolitano C, Gasparini M, Pappone C, Della Bella P, Giordano U, et al. Natural history of Brugada syndrome: insights for risk stratification and management. Circulation. 2002;105:1342–7. - PubMed
-
- Takagi M, Yokoyama Y, Aonuma K, Aihara N, Hiraoka M. Clinical characteristics and risk stratification in symptomatic and asymptomatic patients with brugada syndrome: multicenter study in Japan. J Cardiovasc Electrophysiol. 2007;18:1244–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
