

Melanopsin retinal ganglion cells are resistant to neurodegeneration in mitochondrial optic neuropathies
- PMID: 20659957
- PMCID: PMC3139936
- DOI: 10.1093/brain/awq155
Melanopsin retinal ganglion cells are resistant to neurodegeneration in mitochondrial optic neuropathies
Abstract
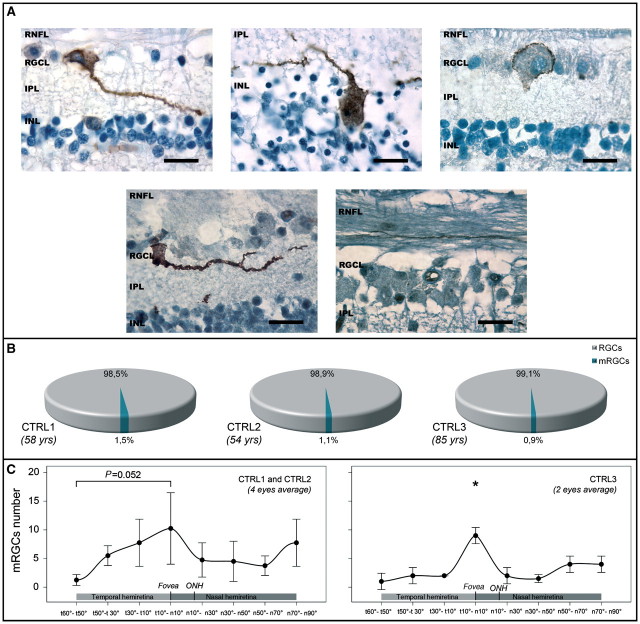
Mitochondrial optic neuropathies, that is, Leber hereditary optic neuropathy and dominant optic atrophy, selectively affect retinal ganglion cells, causing visual loss with relatively preserved pupillary light reflex. The mammalian eye contains a light detection system based on a subset of retinal ganglion cells containing the photopigment melanopsin. These cells give origin to the retinohypothalamic tract and support the non-image-forming visual functions of the eye, which include the photoentrainment of circadian rhythms, light-induced suppression of melatonin secretion and pupillary light reflex. We studied the integrity of the retinohypothalamic tract in five patients with Leber hereditary optic neuropathy, in four with dominant optic atrophy and in nine controls by testing the light-induced suppression of nocturnal melatonin secretion. This response was maintained in optic neuropathy subjects as in controls, indicating that the retinohypothalamic tract is sufficiently preserved to drive light information detected by melanopsin retinal ganglion cells. We then investigated the histology of post-mortem eyes from two patients with Leber hereditary optic neuropathy and one case with dominant optic atrophy, compared with three age-matched controls. On these retinas, melanopsin retinal ganglion cells were characterized by immunohistochemistry and their number and distribution evaluated by a new protocol. In control retinas, we show that melanopsin retinal ganglion cells are lost with age and are more represented in the parafoveal region. In patients, we demonstrate a relative sparing of these cells compared with the massive loss of total retinal ganglion cells, even in the most affected areas of the retina. Our results demonstrate that melanopsin retinal ganglion cells resist neurodegeneration due to mitochondrial dysfunction and maintain non-image-forming functions of the eye in these visually impaired patients. We also show that in normal human retinas, these cells are more concentrated around the fovea and are lost with ageing. The current results provide a plausible explanation for the preservation of pupillary light reaction despite profound visual loss in patients with mitochondrial optic neuropathy, revealing the robustness of melanopsin retinal ganglion cells to a metabolic insult and opening the question of mechanisms that might protect these cells.
Figures



Similar articles
-
The injury resistant ability of melanopsin-expressing intrinsically photosensitive retinal ganglion cells.Neuroscience. 2015 Jan 22;284:845-853. doi: 10.1016/j.neuroscience.2014.11.002. Epub 2014 Nov 10. Neuroscience. 2015. PMID: 25446359 Free PMC article. Review.
-
The pupil light reflex in Leber's hereditary optic neuropathy: evidence for preservation of melanopsin-expressing retinal ganglion cells.Invest Ophthalmol Vis Sci. 2013 Jul 2;54(7):4471-7. doi: 10.1167/iovs.12-11137. Invest Ophthalmol Vis Sci. 2013. PMID: 23737476 Free PMC article.
-
Melanopsin-expressing retinal ganglion cells are resistant to cell injury, but not always.Mitochondrion. 2017 Sep;36:77-84. doi: 10.1016/j.mito.2017.04.003. Epub 2017 Apr 12. Mitochondrion. 2017. PMID: 28412540 Review.
-
Pupillometric evaluation of the melanopsin containing retinal ganglion cells in mitochondrial and non-mitochondrial optic neuropathies.Mitochondrion. 2017 Sep;36:124-129. doi: 10.1016/j.mito.2017.07.003. Epub 2017 Jul 14. Mitochondrion. 2017. PMID: 28716667 Review.
-
Non-image-forming light driven functions are preserved in a mouse model of autosomal dominant optic atrophy.PLoS One. 2013;8(2):e56350. doi: 10.1371/journal.pone.0056350. Epub 2013 Feb 11. PLoS One. 2013. PMID: 23409176 Free PMC article.
Cited by
-
Aging of human short-wave cone pathways.Proc Natl Acad Sci U S A. 2012 Aug 14;109(33):13422-7. doi: 10.1073/pnas.1119770109. Epub 2012 Jul 30. Proc Natl Acad Sci U S A. 2012. PMID: 22847416 Free PMC article.
-
[Leber's hereditary optic neuropathy].Ophthalmologe. 2011 Dec;108(12):1179-92; quiz 1193-4. doi: 10.1007/s00347-011-2482-y. Ophthalmologe. 2011. PMID: 22130685 German.
-
Regulation of Reentrainment Function Is Dependent on a Certain Minimal Number of Intact Functional ipRGCs in rd Mice.J Ophthalmol. 2017;2017:6804853. doi: 10.1155/2017/6804853. Epub 2017 Nov 22. J Ophthalmol. 2017. PMID: 29359039 Free PMC article.
-
Relationship between Daytime Sleepiness and Intrinsically Photosensitive Retinal Ganglion Cells in Glaucomatous Disease.J Ophthalmol. 2016;2016:5317371. doi: 10.1155/2016/5317371. Epub 2016 Feb 3. J Ophthalmol. 2016. PMID: 26955483 Free PMC article.
-
Optic neuropathies: the tip of the neurodegeneration iceberg.Hum Mol Genet. 2017 Oct 1;26(R2):R139-R150. doi: 10.1093/hmg/ddx273. Hum Mol Genet. 2017. PMID: 28977448 Free PMC article. Review.
References
-
- Baver SB, Pickard GE, Sollars PJ, Pickard GE. Two types of melanopsin retinal ganglion cell differentially innervate the hypothalamic suprachiasmatic nucleus and the olivary pretectal nucleus. Eur J Neurosci. 2008;27:1763–70. - PubMed
-
- Berson DM, Dunn FA, Takao M. Phototransduction by retinal ganglion cells that set the circadian clock. Science. 2002;295:1070–3. - PubMed
-
- Bose S, Dhillon N, Ross-Cisneros FN, Carelli V. Relative post-mortem sparing of afferent pupil fibers in a patient with 3460 Leber's hereditary optic neuropathy. Graefes Arch Clin Exp Ophthalmol. 2005;243:1175–9. - PubMed
-
- Bremner FD, Shallo-Hoffmann J, Riordan-Eva P, Smith SE. Comparing pupil function with visual function in patients with Leber's hereditary optic neuropathy. Invest Ophthalmol Vis Sci. 1999;40:2528–34. - PubMed
