

Reducing wasting in young children with preventive supplementation: a cohort study in Niger
- PMID: 20660552
- PMCID: PMC3144628
- DOI: 10.1542/peds.2009-2814
Reducing wasting in young children with preventive supplementation: a cohort study in Niger
Abstract
Objective: To compare the incidence of wasting, stunting, and mortality among children aged 6 to 36 months who are receiving preventive supplementation with either ready-to-use supplementary foods (RUSFs) or ready-to-use therapeutic foods (RUTFs).
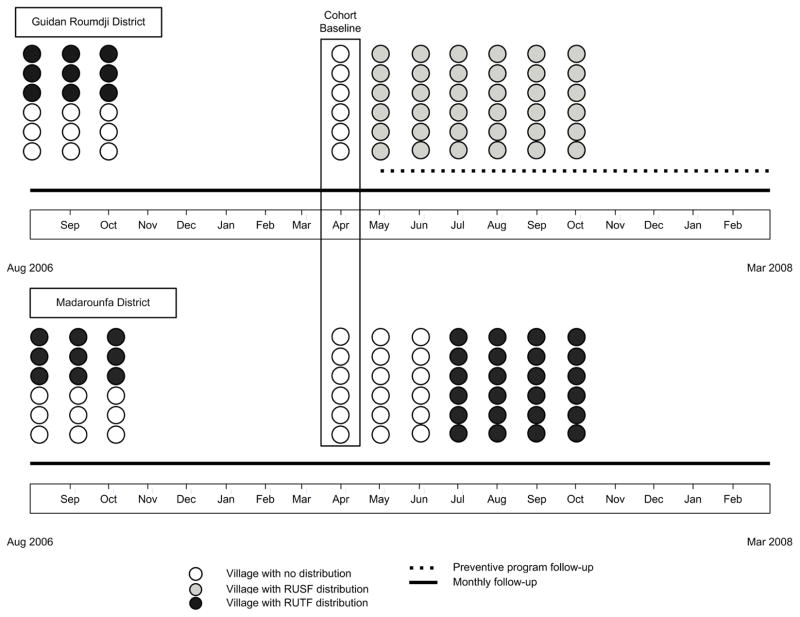
Subjects and methods: Children aged 6 to 36 months in 12 villages of Maradi, Niger, (n = 1645) received a monthly distribution of RUSFs (247 kcal [3 spoons] per day) for 6 months or RUTFs (500-kcal sachet per day) for 4 months. We compared the incidence of wasting, stunting, and mortality among children who received preventive supplementation with RUSFs versus RUTFs.
Results: The effectiveness of RUSF supplementation depended on receipt of a previous preventive intervention. In villages in which a preventive supplementation program was previously implemented, the RUSF strategy was associated with a 46% (95% confidence interval [CI]: 6%-69%) and 59% (95% CI: 17%-80%) reduction in wasting and severe wasting, respectively. In contrast, in villages in which the previous intervention was not implemented, we found no difference in the incidence of wasting or severe wasting according to type of supplementation. Compared with the RUTF strategy, the RUSF strategy was associated with a 19% (95% CI: 0%-34%) reduction in stunting overall.
Conclusion: We found that the relative performance of a 6-month RUSF supplementation strategy versus a 4-month RUTF strategy varied with receipt of a previous nutritional intervention. Contextual factors will continue to be important in determining the dose and duration of supplementation that will be most effective, acceptable, and sustainable for a given setting.
Conflict of interest statement
Figures
References
-
- Ciliberto MA, Sandige H, Ndekha MJ, et al. Comparison of home-based therapy with ready-to-use therapeutic food with standard therapy in the treatment of malnourished Malawian children: a controlled, clinical effectiveness trial. Am J Clin Nutr. 2005;81(4):864–70. - PubMed
-
- Diop el HI, Dossou NI, Ndour MM, Briend A, Wade S. Comparison of the efficacy of a solid ready-to-use food and a liquid, milk-based diet for the rehabilitation of severely malnourished children: a randomized trial. Am J Clin Nutr. 2003;78(2):302–7. - PubMed
-
- Ndekha MJ, Manary MJ, Ashorn P, Briend A. Home-based therapy with ready-to-use therapeutic food is of benefit to malnourished, HIV-infected Malawian children. Acta Paediatr. 2005;94(2):222–5. - PubMed
-
- World Health Organization, World Food Programme, United Nations System Standing Committee on Nutrition and United Nations Children’s Fund. Community-Based Management of Severe Acute Malnutrition. Geneva, Rome, New York: WHO, WFP, SCN and UNICEF; 2007.
