

Quantifying cost-effectiveness of controlling nosocomial spread of antibiotic-resistant bacteria: the case of MRSA
- PMID: 20661278
- PMCID: PMC2905392
- DOI: 10.1371/journal.pone.0011562
Quantifying cost-effectiveness of controlling nosocomial spread of antibiotic-resistant bacteria: the case of MRSA
Abstract
Background: The costs and benefits of controlling nosocomial spread of antibiotic-resistant bacteria are unknown.
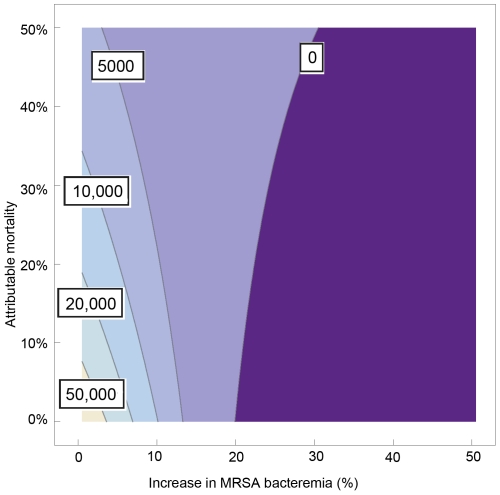
Methods: We developed a mathematical algorithm to determine cost-effectiveness of infection control programs and explored the dynamical interactions between different epidemiological variables and cost-effectiveness. The algorithm includes occurrence of nosocomial infections, attributable mortality, costs and efficacy of infection control and how antibiotic-resistant bacteria affect total number of infections: do infections with antibiotic-resistant bacteria replace infections caused by susceptible bacteria (replacement scenario) or occur in addition to them (addition scenario). Methicillin-resistant Staphylococcus aureus (MRSA) bacteremia was used for illustration using observational data on S. aureus bacteremia (SAB) in our hospital (n = 189 between 2001-2004, all being methicillin-susceptible S. aureus [MSSA]).
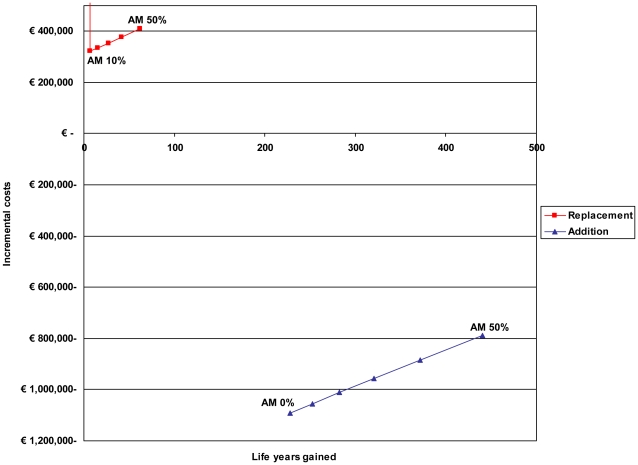
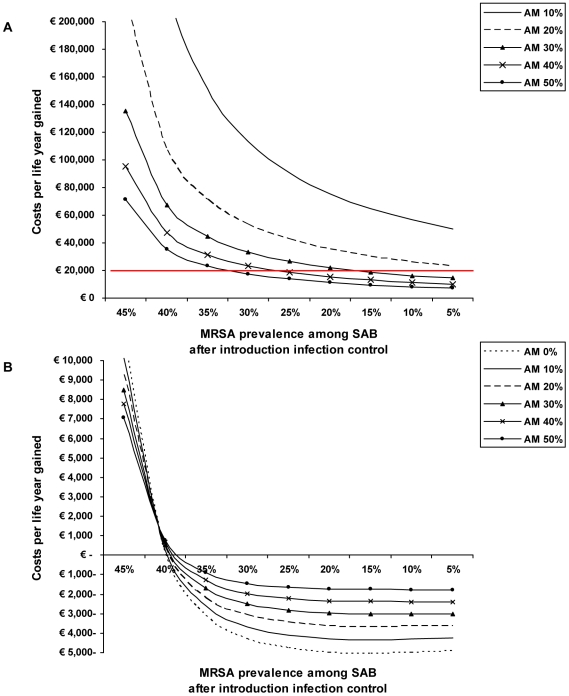
Results: In the replacement scenario, the costs per life year gained range from 45,912 euros to 6590 euros for attributable mortality rates ranging from 10% to 50%. Using 20,000 euros per life year gained as a threshold, completely preventing MRSA would be cost-effective in the replacement scenario if attributable mortality of MRSA is > or = 21%. In the addition scenario, infection control would be cost saving along the entire range of estimates for attributable mortality.
Conclusions: Cost-effectiveness of controlling antibiotic-resistant bacteria is highly sensitive to the interaction between infections caused by resistant and susceptible bacteria (addition or replacement) and attributable mortality. In our setting, controlling MRSA would be cost saving for the addition scenario but would not be cost-effective in the replacement scenario if attributable mortality would be < 21%.
Conflict of interest statement
Figures
References
-
- Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, et al. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis. 2003;36:53–59. - PubMed
-
- Reed SD, Friedman JY, Engemann JJ, Griffiths RI, Anstrom KJ, et al. Costs and outcomes among hemodialysis-dependent patients with methicillin-resistant or methicillin-susceptible Staphylococcus aureus bacteremia. Infect Control Hosp Epidemiol. 2005;26:175–183. - PubMed
-
- Engemann JJ, Carmeli Y, Cosgrove SE, Fowler VG, Bronstein MZ, et al. Adverse clinical and economic outcomes attributable to methicillin resistance among patients with Staphylococcus aureus surgical site infection. Clin Infect Dis. 2003;36:592–598. - PubMed
-
- Cosgrove SE, Qi Y, Kaye KS, Harbarth S, Karchmer AW, et al. The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges. Infect Control Hosp Epidemiol. 2005;26:166–174. - PubMed
-
- RIVM. European Antimicrobial Resistance Surveillance System. 2005. Available: http://www.rivm.nl/earss/database/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
