

Clinically relevant characterization of lung adenocarcinoma subtypes based on cellular pathways: an international validation study
- PMID: 20661423
- PMCID: PMC2908611
- DOI: 10.1371/journal.pone.0011712
Clinically relevant characterization of lung adenocarcinoma subtypes based on cellular pathways: an international validation study
Abstract
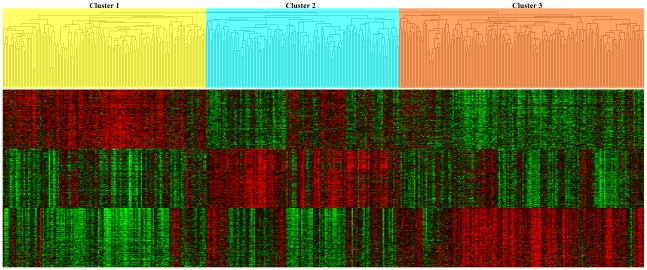
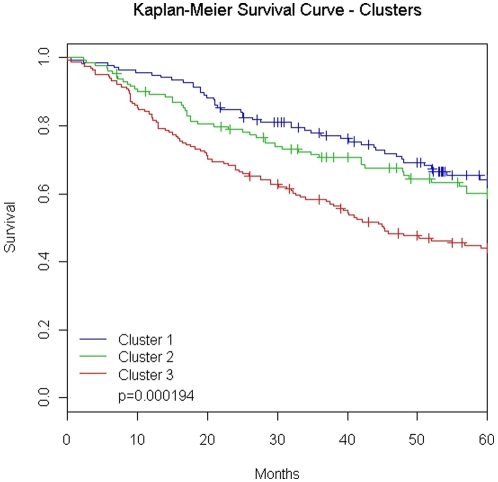
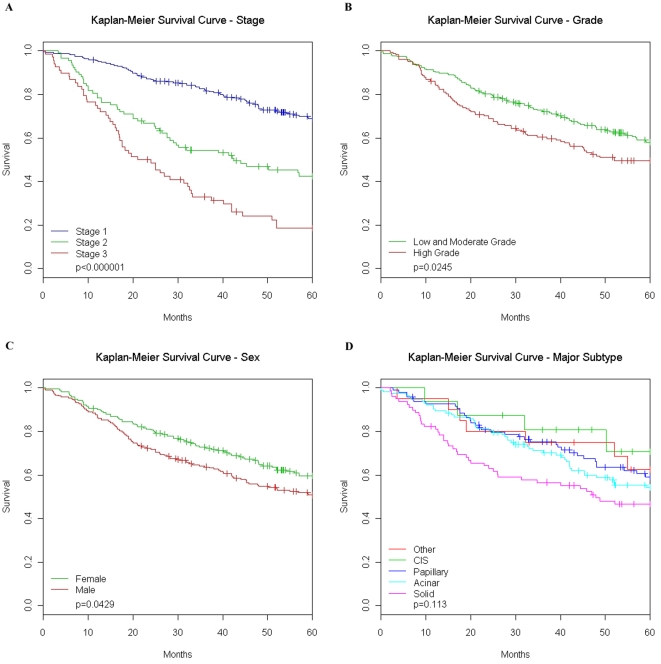
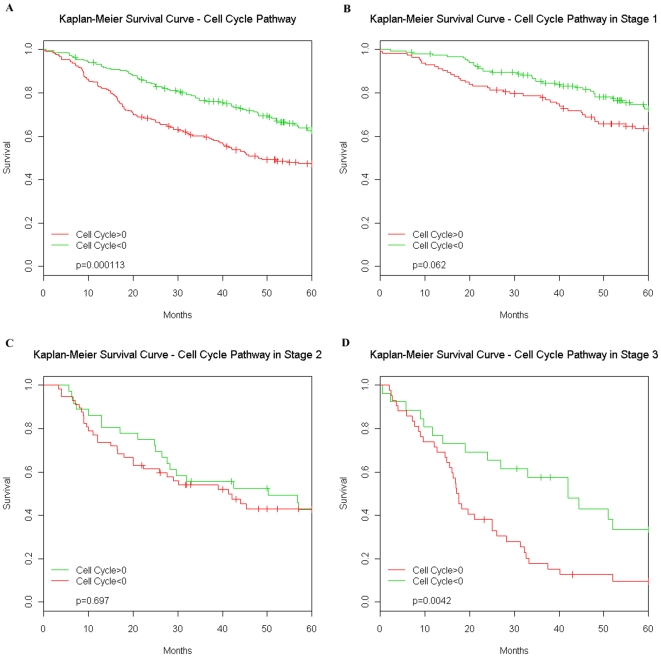
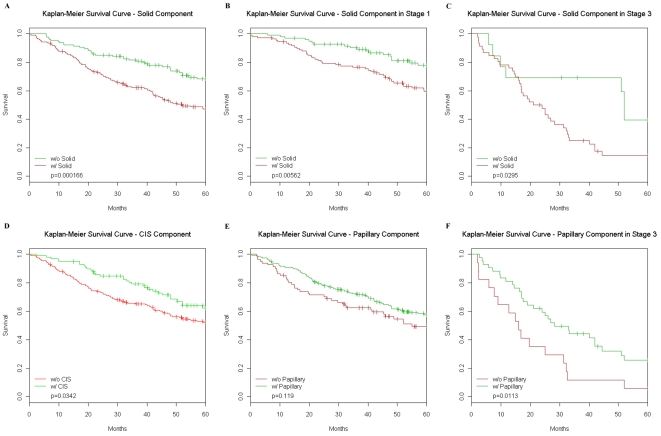
Lung adenocarcinoma (AD) represents a predominant type of lung cancer demonstrating significant morphologic and molecular heterogeneity. We sought to understand this heterogeneity by utilizing gene expression analyses of 432 AD samples and examining associations between 27 known cancer-related pathways and the AD subtype, clinical characteristics and patient survival. Unsupervised clustering of AD and gene expression enrichment analysis reveals that cell proliferation is the most important pathway separating tumors into subgroups. Further, AD with increased cell proliferation demonstrate significantly poorer outcome and an increased solid AD subtype component. Additionally, we find that tumors with any solid component have decreased survival as compared to tumors without a solid component. These results lead to the potential to use a relatively simple pathological examination of a tumor in order to determine its aggressiveness and the patient's prognosis. Additional results suggest the ability to use a similar approach to determine a patient's sensitivity to targeted treatment. We then demonstrated the consistency of these findings using two independent AD cohorts from Asia (N = 87) and Europe (N = 89) using the identical analytic procedures.
Conflict of interest statement
Figures
References
-
- Jemal A, Clegg LX, Ward E, Ries LA, Wu X, et al. Annual report to the nation on the status of cancer, 1975-2001, with a special feature regarding survival. Cancer. 2004;101:3–27. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
