

Increased pulmonary pressures and myocardial wall stress in children with severe malaria
- PMID: 20662718
- PMCID: PMC3206728
- DOI: 10.1086/655225
Increased pulmonary pressures and myocardial wall stress in children with severe malaria
Abstract
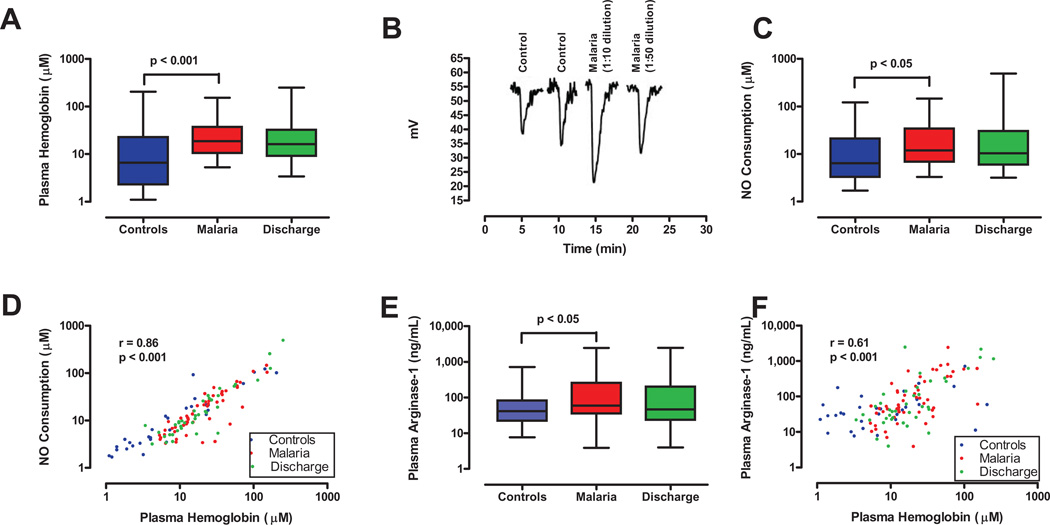
Background: Chronic intravascular hemolysis leads to nitric oxide (NO) depletion and pulmonary hypertension in sickle cell disease. To test whether this pathophysiology occurs in malaria, we examined in Mali 53 children who were admitted to the hospital with severe malaria (excluding cerebral malaria) and 31 age-matched controls.
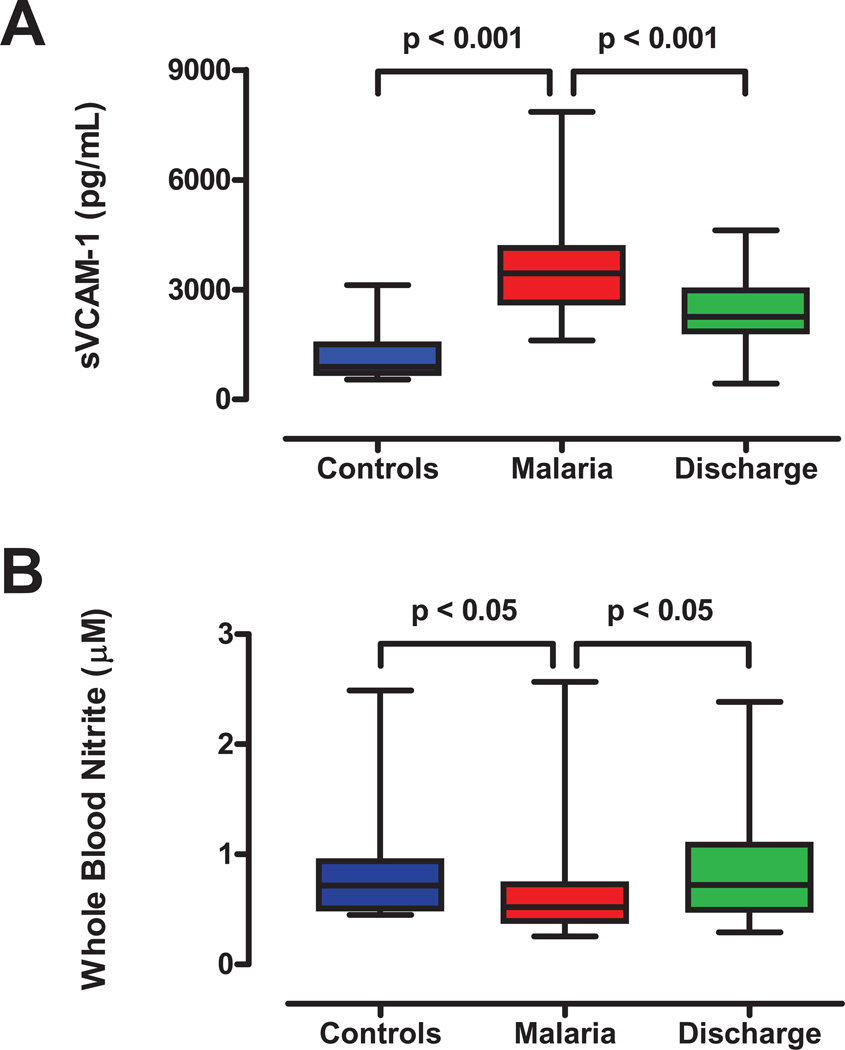
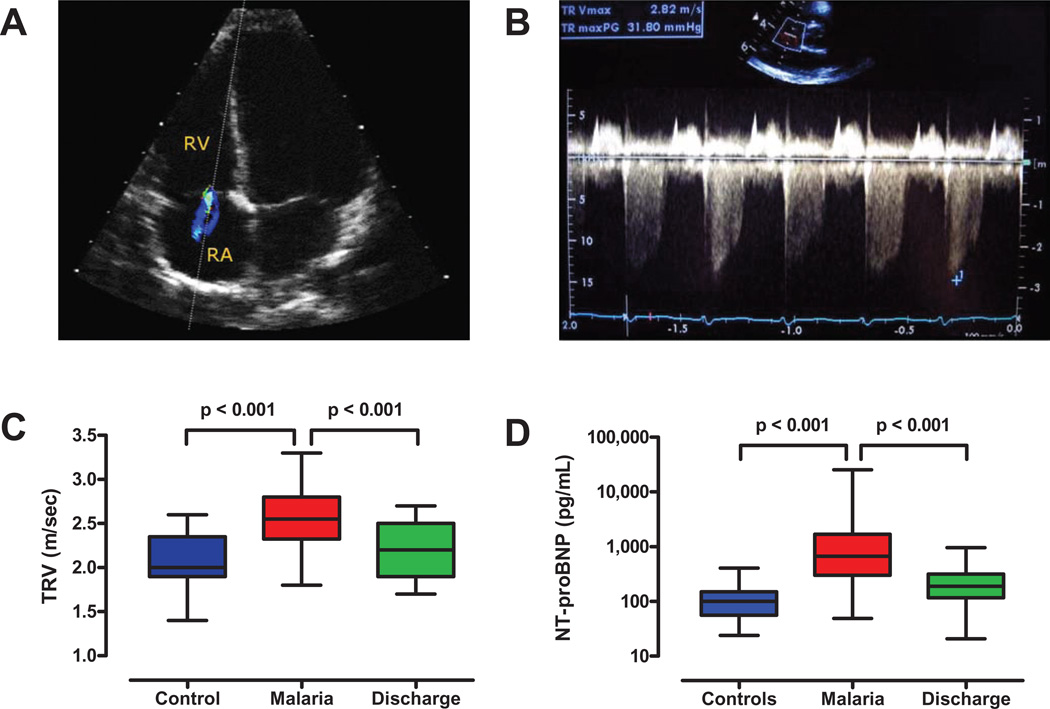
Methods: Severity of hemolysis was assessed from plasma levels of free hemoglobin and arginase-1. NO metabolism was assessed by whole-blood nitrite levels and plasma NO consumption. Effects on the cardiovascular system and endothelial function were assessed by using echocardiography to measure peak tricuspid regurgitant jet velocity and by evaluating plasma levels of N-terminal prohormone brain natriuretic peptide (NT-proBNP) and soluble vascular cell adhesion molecule-1.
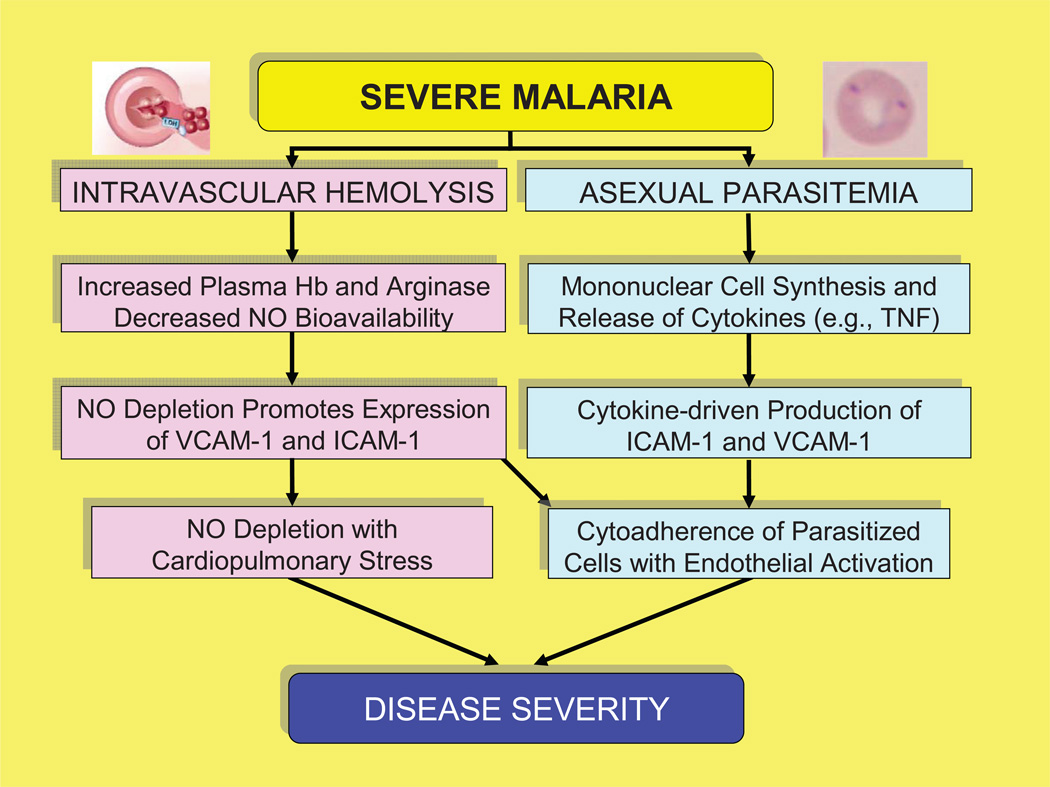
Results: Children with severe malaria had higher plasma levels of hemoglobin and arginase-1, reduced whole-blood levels of nitrite, and increased NO consumption relative to controls. They also had increased pulmonary arterial pressures (P< .05) with elevated levels of NT-proBNP and soluble vascular cell adhesion molecule-1 (P< .001).
Conclusion: Children with severe malaria have increased pulmonary pressures and myocardial wall stress. These complications are consistent with NO depletion from intravascular hemolysis, and they indicate that the pathophysiologic cascade from intravascular hemolysis to NO depletion and its cardiopulmonary effects is activated in children with severe malaria.
Conflict of interest statement
Conflict of Interest
The authors declare that they do not have commercial or other associations that might pose a conflict of interest.
Figures
References
-
- Laveran CL. Classics in infectious diseases: A newly discovered parasite in the blood of patients suffering from malaria. Parasitic etiology of attacks of malaria: Charles Louis Alphonse Laveran (1845–1922) Rev Infect Dis. 1982;4(4):908–911. - PubMed
-
- Geneva: World Health Organization; 2009. [Accessed 26 February 2010]. Roll Back Malaria: Global Malaria Action Plan: Key Facts, Figures and Strategies. Available at: http://www.rollbackmalaria.org/gmap/.
-
- Korenromp EL, Williams BG, Gouws E, Dye C, Snow RW. Measurement of trends in childhood malaria mortality in Africa: an assessment of progress toward targets based on verbal autopsy. Lancet Infect Dis. 2003;3:349–358. - PubMed
-
- Pasvol G. Treatment of complicated and severe malaria. Br Med Bull. 2005;75–76:29–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
