

Targeted exercise against osteoporosis: A systematic review and meta-analysis for optimising bone strength throughout life
- PMID: 20663158
- PMCID: PMC2918523
- DOI: 10.1186/1741-7015-8-47
Targeted exercise against osteoporosis: A systematic review and meta-analysis for optimising bone strength throughout life
Abstract
Background: Exercise is widely recommended to reduce osteoporosis, falls and related fragility fractures, but its effect on whole bone strength has remained inconclusive. The primary purpose of this systematic review and meta-analysis was to evaluate the effects of long-term supervised exercise (> or =6 months) on estimates of lower-extremity bone strength from childhood to older age.
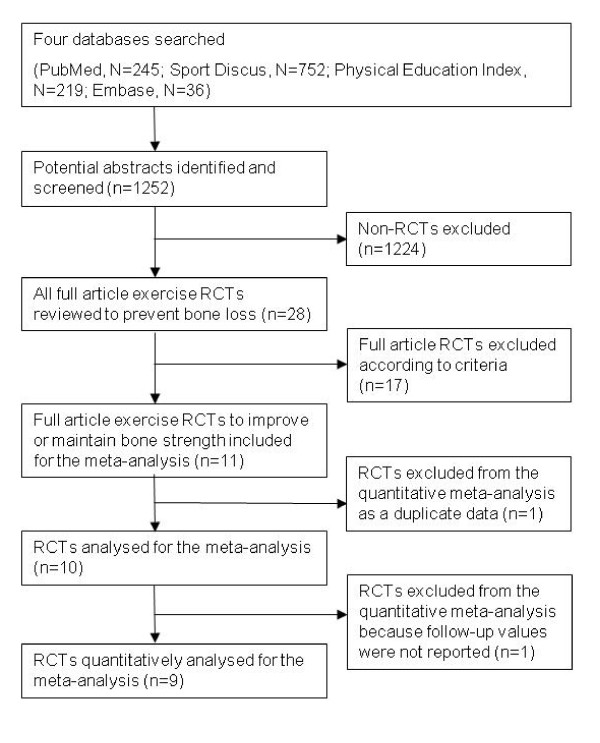
Methods: We searched four databases (PubMed, Sport Discus, Physical Education Index, and Embase) up to October 2009 and included 10 randomised controlled trials (RCTs) that assessed the effects of exercise training on whole bone strength. We analysed the results by age groups (childhood, adolescence, and young and older adulthood) and compared the changes to habitually active or sedentary controls. To calculate standardized mean differences (SMD; effect size), we used the follow-up values of bone strength measures adjusted for baseline bone values. An inverse variance-weighted random-effects model was used to pool the results across studies.
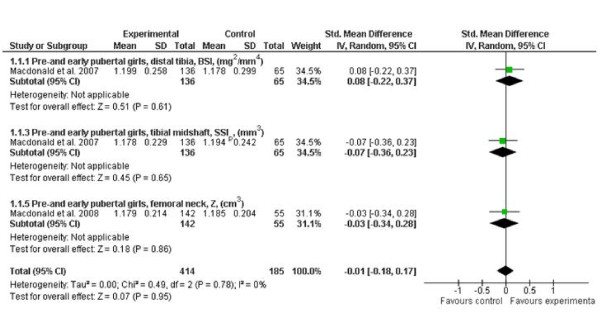
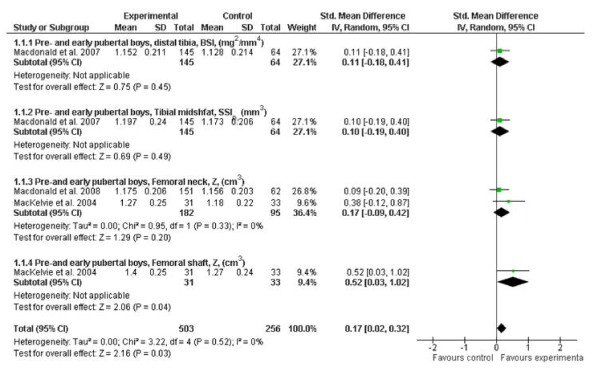
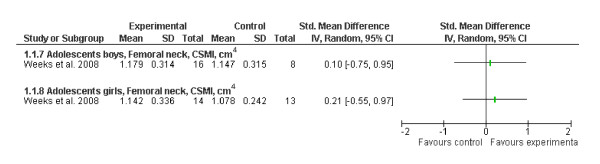
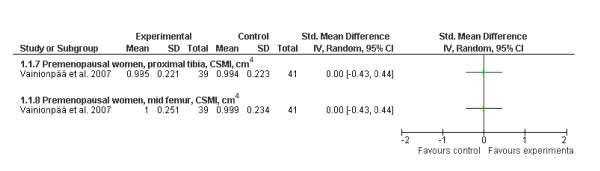
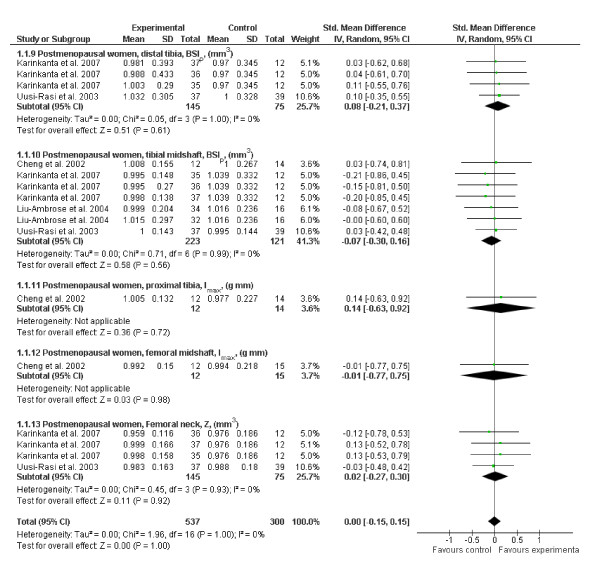
Results: Our quality analysis revealed that exercise regimens were heterogeneous; some trials were short in duration and small in sample size, and the weekly training doses varied considerably between trials. We found a small and significant exercise effect among pre- and early pubertal boys [SMD, effect size, 0.17 (95% CI, 0.02-0.32)], but not among pubertal girls [-0.01 (-0.18 to 0.17)], adolescent boys [0.10 (-0.75 to 0.95)], adolescent girls [0.21 (-0.53 to 0.97)], premenopausal women [0.00 (-0.43 to 0.44)] or postmenopausal women [0.00 (-0.15 to 0.15)]. Evidence based on per-protocol analyses of individual trials in children and adolescents indicated that programmes incorporating regular weight-bearing exercise can result in 1% to 8% improvements in bone strength at the loaded skeletal sites. In premenopausal women with high exercise compliance, improvements ranging from 0.5% to 2.5% have been reported.
Conclusions: The findings from our meta-analysis of RCTs indicate that exercise can significantly enhance bone strength at loaded sites in children but not in adults. Since few RCTs were conducted to investigate exercise effects on bone strength, there is still a need for further well-designed, long-term RCTs with adequate sample sizes to quantify the effects of exercise on whole bone strength and its structural determinants throughout life.
Figures
References
-
- US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, MD, US Department of Health and Human Services, Office of the Surgeon General. 2004.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
