

Impact of hyperglycemia on morbidity and mortality, length of hospitalization and rates of re-hospitalization in a general hospital setting in Brazil
- PMID: 20663179
- PMCID: PMC2912825
- DOI: 10.1186/1758-5996-2-49
Impact of hyperglycemia on morbidity and mortality, length of hospitalization and rates of re-hospitalization in a general hospital setting in Brazil
Abstract
Background: Hyperglycemia in hospitalized patients is known to be related to a higher incidence of clinical and surgical complications and poorer outcomes. Adequate glycemic control and earlier diagnosis of type 2 diabetes during hospitalization are cost-effective measures.
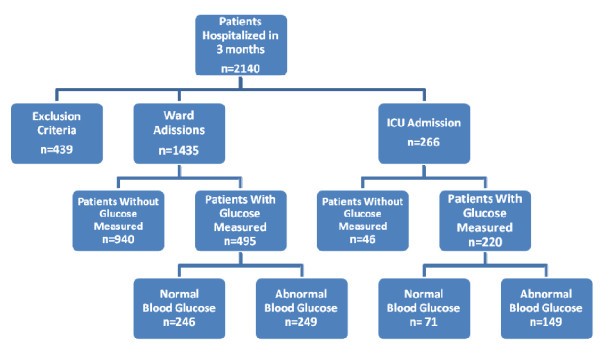
Methods: This prospective cohort study was designed to determine the impact of hyperglycemia on morbidity and mortality in a general hospital setting during a 3-month period by reviewing patients' records. The primary purposes of this trial were to verify that hyperglycemia was diagnosed properly and sufficiently early and that it was managed during the hospital stay; we also aimed to evaluate the relationship between in-hospital hyperglycemia control and outcomes such as complications during the hospital stay, extent of hospitalization, frequency of re-hospitalization, death rates and number of days in the ICU (Intensive Care Unit) after admission. Statistical analyses utilized the Kruskall-Wallis complemented by the "a posteriori" d.m.s. test, Spearman correlation and Chi-squared test, with a level of significance of 5% (p < 0.05).
Results: We reviewed 779 patient records that fulfilled inclusion criteria. The patients were divided into 5 groups: group (1) diabetic with normal glycemic levels according to American Diabetes Association criteria for in-hospital patients (n = 123); group (2) diabetics with hyperglycemia (n = 76); group (3) non-diabetics with hyperglycemia (n = 225); group (4)diabetics and non-diabetics with persistent hyperglycemia during 3 consecutive days (n = 57) and group (5) those with normal glucose control (n = 298). Compared to patients in groups 1 and 5, patients in groups 2, 3 and 4 had significantly higher mortality rates (17.7% vs. 2.8%) and Intensive Care Unit admissions with complications (23.3% vs. 4.5%). Patients in group 4 had the longest hospitalizations (mean 15.5 days), and group 5 had the lowest re-hospitalization rate (mean of 1.28 hospitalizations). Only 184 (51.4%) hyperglycemic patients had received treatment. An insulin "sliding-scale" alone was the most frequent treatment used, and there was a wide variation in glucose target medical prescriptions. Intra Venous insulin infusion was used in 3.8% of patients in the ICU. Glycohemoglobin(A1C) was measured in 11 patients(2.2%).
Conclusions: Hospital hyperglycemia was correlated with, among other parameters, morbidity/mortality, length of hospitalization and number of re-hospitalizations. Most patients did not have their glycemic levels measured at the hospital; despite the high number of hyperglycemic patients not diagnosed as diabetics, A1C was not frequently measured. Even when patients are assessed for hyperglycemia, they were not treated properly.
Figures
Similar articles
-
Prognostic impact of in-hospital hyperglycemia in hospitalized patients with acute heart failure: Results of the IN-HF (Italian Network on Heart Failure) Outcome registry.Int J Cardiol. 2016 Jan 15;203:587-93. doi: 10.1016/j.ijcard.2015.10.207. Epub 2015 Nov 11. Int J Cardiol. 2016. PMID: 26574932
-
IMPACT OF GLUCOSE MANAGEMENT TEAM ON OUTCOMES OF HOSPITALIZARON IN PATIENTS WITH TYPE 2 DIABETES ADMITTED TO THE MEDICAL SERVICE.Endocr Pract. 2016 Dec;22(12):1401-1405. doi: 10.4158/EP161414.OR. Epub 2016 Aug 19. Endocr Pract. 2016. PMID: 27540884
-
Addressing hyperglycemia from hospital admission to discharge.Curr Med Res Opin. 2010 Mar;26(3):589-98. doi: 10.1185/03007990903566822. Curr Med Res Opin. 2010. PMID: 20078323 Review.
-
Influence of diabetes and hyperglycemia on duration of stay in patients hospitalized with congestive heart failure.Endocr Pract. 2008 Sep;14(6):691-6. doi: 10.4158/EP.14.6.691. Endocr Pract. 2008. PMID: 18996787
-
Hyperglycemia in the hospital setting: the case for improved control among non-diabetics.Ann Pharmacother. 2005 Mar;39(3):492-501. doi: 10.1345/aph.1E308. Epub 2005 Feb 8. Ann Pharmacother. 2005. PMID: 15701779 Review.
Cited by
-
Correlation Between Hemoglobin A1c (HbA1c) and High-Sensitivity C-Reactive Protein (hs-CRP) in Myocardial Infarction Patients and Their Six-Month Mortality Follow-Up.Cureus. 2024 Aug 17;16(8):e67070. doi: 10.7759/cureus.67070. eCollection 2024 Aug. Cureus. 2024. PMID: 39286672 Free PMC article.
-
Validation of Diagnostic Coding for Diabetes Mellitus in Hospitalized Patients.Endocr Pract. 2022 May;28(5):458-464. doi: 10.1016/j.eprac.2022.01.014. Epub 2022 Feb 4. Endocr Pract. 2022. PMID: 35131439 Free PMC article.
-
A systematic scoping review on the consequences of stress-related hyperglycaemia.PLoS One. 2018 Apr 6;13(4):e0194952. doi: 10.1371/journal.pone.0194952. eCollection 2018. PLoS One. 2018. PMID: 29624594 Free PMC article.
-
Effect of informatization-based blood glucose team management on the control of hyperglycaemia in noncritical care units.PLoS One. 2020 Mar 11;15(3):e0230115. doi: 10.1371/journal.pone.0230115. eCollection 2020. PLoS One. 2020. PMID: 32160260 Free PMC article.
-
Inpatient hyperglycaemia, and impact on morbidity, mortality and re-hospitalisation rates.Clin Med (Lond). 2022 Jul;22(4):325-331. doi: 10.7861/clinmed.2022-0112. Clin Med (Lond). 2022. PMID: 35882487 Free PMC article.
References
-
- Vanhorebeek I, Langouche L, Berghe GVD. Intensive Insulin Therapy in the Intensive Care Unit: Update on Clinical Impact and Mechanisms of Action. Endocrine Practice. 2006;12(Suppl 3):14–22. - PubMed
-
- Kitabchi AE, Freire AX, Umpierrez GE. Evidence for strict inpatient glycemic control: time to revise glycemic goals in hospitalized patients. Metabolism Clinical and Experimental. 2008;57:116–120. - PubMed
-
- ACE/ADA Task Force on Inpatient Diabetes. American College of Endocrinology and American Diabetes Association Consensus Statement on Inpatient Diabetes and Glycemic Control. Endocrine Practice. 2006;12(Suppl 4):458–468. - PubMed
-
- Thompson CL, Dunn KC, Menon MC, Kearns LE, Braithwaite SB. Hyperglycemia in the Hospital. Diabetes Spectrum. 2005;18(Suppl 1):20–27. doi: 10.2337/diaspect.18.1.20. - DOI
LinkOut - more resources
Full Text Sources
