

Epidemiology and control of intestinal schistosomiasis on the Sesse Islands, Uganda: integrating malacology and parasitology to tailor local treatment recommendations
- PMID: 20663223
- PMCID: PMC2920240
- DOI: 10.1186/1756-3305-3-64
Epidemiology and control of intestinal schistosomiasis on the Sesse Islands, Uganda: integrating malacology and parasitology to tailor local treatment recommendations
Abstract
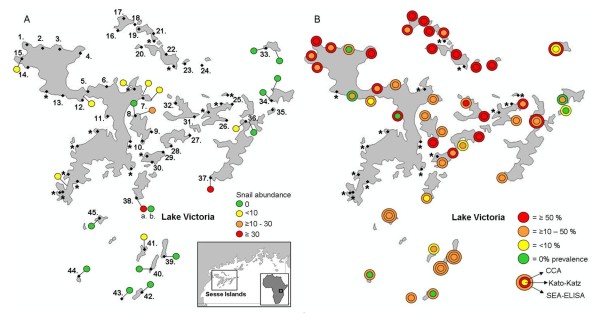
Background: Intestinal schistosomiasis is often widespread among the populations living around Lake Victoria and on its islands. The Sesse Island group (containing some 84 islands), however, is typically assumed to be a low prevalence zone, with limited transmission, but has never been surveyed in detail. Here, we present a rapid mapping assessment, bringing together snail and parasite information, at 23 sites for the presence of intermediate host snails and at 61 sites for the prevalence of intestinal schistosomiasis in school-aged children (N = 905). Two different diagnostic tools were used and compared at 45 of these sites: Kato-Katz thick faecal smears and circulating cathodic antigen (CCA) urine dipsticks.
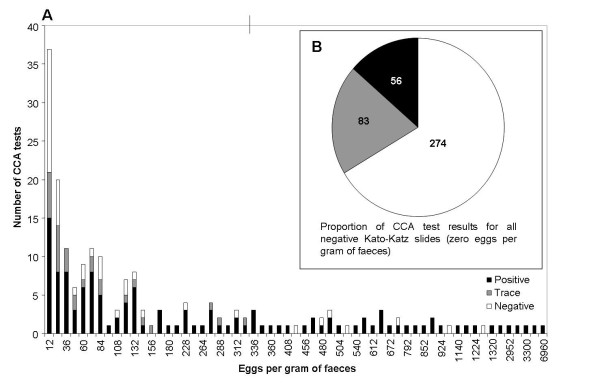
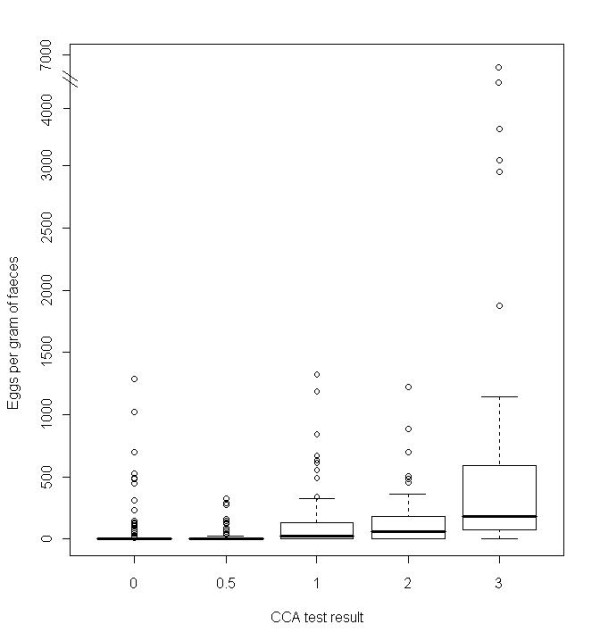
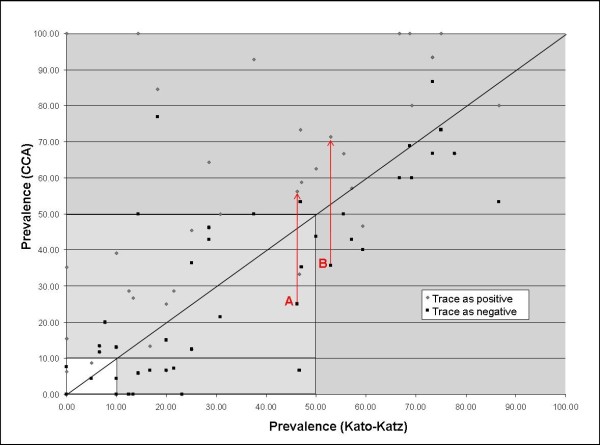
Results: Biomphalaria snails were found at 11 sites but in low numbers; none was found shedding schistosome cercariae. At 22 out of the 45 sites, local prevalence by urine and/or stool diagnostics was in excess of 50%, although mean prevalence of intestinal schistosomiasis overall was 34.6% (95% confidence intervals (CI) = 31.0-38.3%) by Kato-Katz and 46.5% (95% CI = 42.7-50.4%) by CCA if 'trace' reactions were considered infection-positive (if considered infection-negative, mean prevalence was 28.1% (95% CI = 24.7-31.7%)). Diagnostic congruence between CCA and Kato-Katz was poor and significant discordance in estimated prevalence by location was found, with each often inferring different mass drug administration regimes.
Conclusions: Accurate estimation of schistosome prevalence is important for determining present and future treatment needs with praziquantel; the wide range of schistosome prevalence across the Sesse Island group requires a treatment regime largely tailored to each island. In high prevalence locations, further malacological sampling is required to confirm the extent of local transmission, especially on the northern islands within the group. The observation that different diagnostic tests can provide varying results in terms of estimating prevalence by location, and hence change treatment recommendations, suggests that care must be taken in interpreting raw prevalence data. In particular, further research into the reasons for the differences in the poorer performance of the CCA test should be pursued.
Figures
Similar articles
-
Performance of circulating cathodic antigen (CCA) urine-dipsticks for rapid detection of intestinal schistosomiasis in schoolchildren from shoreline communities of Lake Victoria.Parasit Vectors. 2010 Feb 5;3(1):7. doi: 10.1186/1756-3305-3-7. Parasit Vectors. 2010. PMID: 20181101 Free PMC article.
-
Detecting Schistosoma mansoni infections among pre-school-aged children in southern Ghana: a diagnostic comparison of urine-CCA, real-time PCR and Kato-Katz assays.BMC Infect Dis. 2020 Apr 22;20(1):301. doi: 10.1186/s12879-020-05034-2. BMC Infect Dis. 2020. PMID: 32321418 Free PMC article.
-
Intestinal schistosomiasis in Uganda at high altitude (>1400 m): malacological and epidemiological surveys on Mount Elgon and in Fort Portal crater lakes reveal extra preventive chemotherapy needs.Infect Dis Poverty. 2017 Feb 6;6(1):34. doi: 10.1186/s40249-017-0248-8. Infect Dis Poverty. 2017. PMID: 28162096 Free PMC article.
-
Evaluation of circulating cathodic antigen (CCA) urine-cassette assay as a survey tool for Schistosoma mansoni in different transmission settings within Bugiri District, Uganda.Acta Trop. 2014 Aug;136:50-7. doi: 10.1016/j.actatropica.2014.04.001. Epub 2014 Apr 12. Acta Trop. 2014. PMID: 24727052
-
Schistosomiasis is more prevalent than previously thought: what does it mean for public health goals, policies, strategies, guidelines and intervention programs?Infect Dis Poverty. 2017 Mar 22;6(1):63. doi: 10.1186/s40249-017-0275-5. Infect Dis Poverty. 2017. PMID: 28327187 Free PMC article. Review.
Cited by
-
Compensatory density feedback of Oncomelania hupensis populations in two different environmental settings in China.Parasit Vectors. 2011 Jul 13;4:133. doi: 10.1186/1756-3305-4-133. Parasit Vectors. 2011. PMID: 21752244 Free PMC article.
-
Confirmed local endemicity and putative high transmission of Schistosoma mansoni in the Sesse Islands, Lake Victoria, Uganda.Parasit Vectors. 2011 Mar 1;4:29. doi: 10.1186/1756-3305-4-29. Parasit Vectors. 2011. PMID: 21362166 Free PMC article.
-
Surveillance of intestinal schistosomiasis during control: a comparison of four diagnostic tests across five Ugandan primary schools in the Lake Albert region.Parasitology. 2018 Nov;145(13):1715-1722. doi: 10.1017/S003118201800029X. Epub 2018 Mar 21. Parasitology. 2018. PMID: 29560841 Free PMC article.
-
Dynamics of freshwater snails and Schistosoma infection prevalence in schoolchildren during the construction and operation of a multipurpose dam in central Côte d'Ivoire.Infect Dis Poverty. 2017 May 4;6(1):93. doi: 10.1186/s40249-017-0305-3. Infect Dis Poverty. 2017. PMID: 28468667 Free PMC article.
-
Comparison of Schistosoma mansoni Prevalence and Intensity of Infection, as Determined by the Circulating Cathodic Antigen Urine Assay or by the Kato-Katz Fecal Assay: A Systematic Review.Am J Trop Med Hyg. 2016 Mar;94(3):605-610. doi: 10.4269/ajtmh.15-0725. Epub 2016 Jan 11. Am J Trop Med Hyg. 2016. PMID: 26755565 Free PMC article.
References
-
- Brooker S, Kabatereine NB, Myatt M, Stothard JR, Fenwick A. Rapid assessment of Schistosoma mansoni: the validity, applicability and cost-effectiveness of the Lot Quality Assurance Sampling method in Uganda. Trop Med Int Health. 2005;10:647–658. doi: 10.1111/j.1365-3156.2005.01446.x. - DOI - PMC - PubMed
-
- Standley CJ, Lwambo N, Lange C, Kariuki H, Adriko M, Stothard JR. Performance of circulating cathodic antigen (CCA) urine-dipsticks for rapid detection of intestinal schistosomiasis in schoolchildren from shoreline communities of Lake Victoria. Parasit Vectors. 2010;3:7. doi: 10.1186/1756-3305-3-7. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
