

Wyburn-Mason or Bonnet-Dechaume-Blanc as Cerebrofacial Arteriovenous Metameric Syndromes (CAMS). A New Concept and a New Classification
- PMID: 20663326
- PMCID: PMC3621461
- DOI: 10.1177/159101990100700101
Wyburn-Mason or Bonnet-Dechaume-Blanc as Cerebrofacial Arteriovenous Metameric Syndromes (CAMS). A New Concept and a New Classification
Abstract
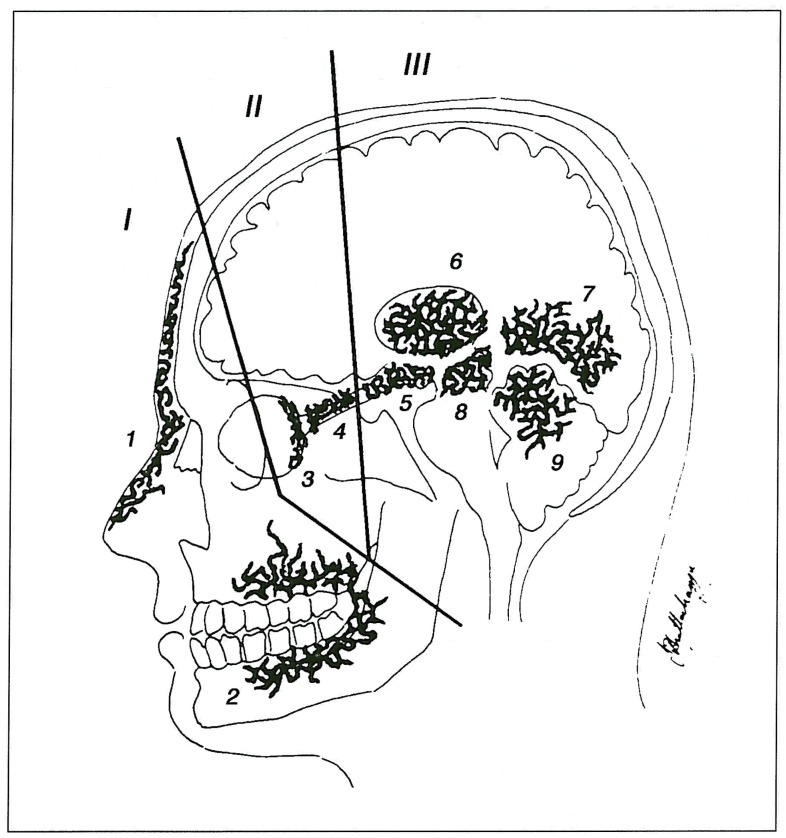
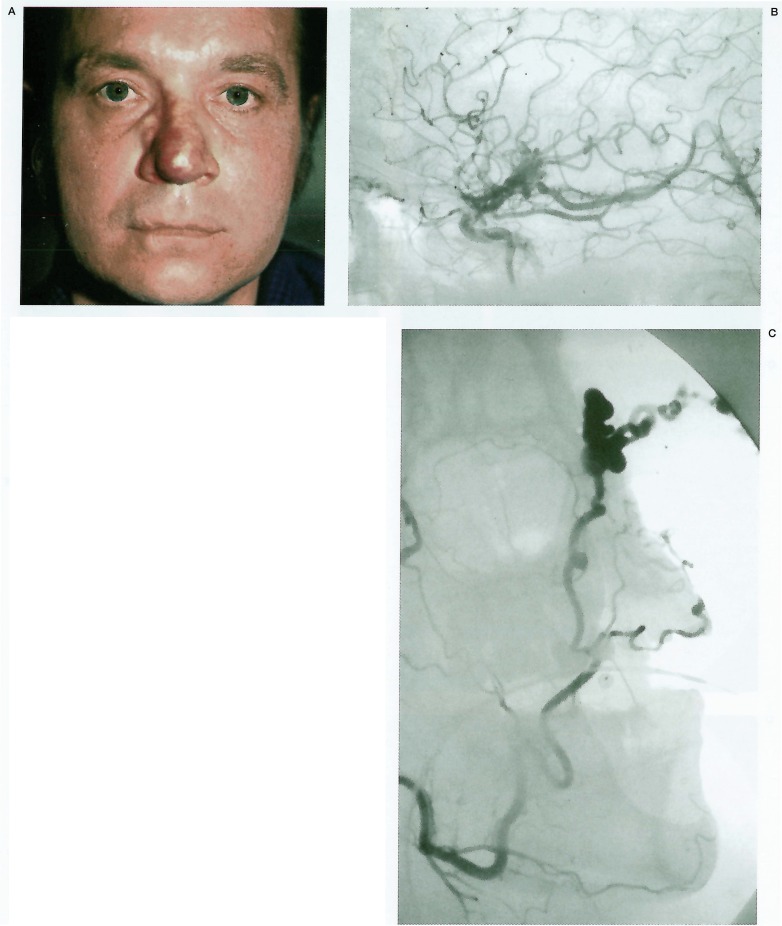
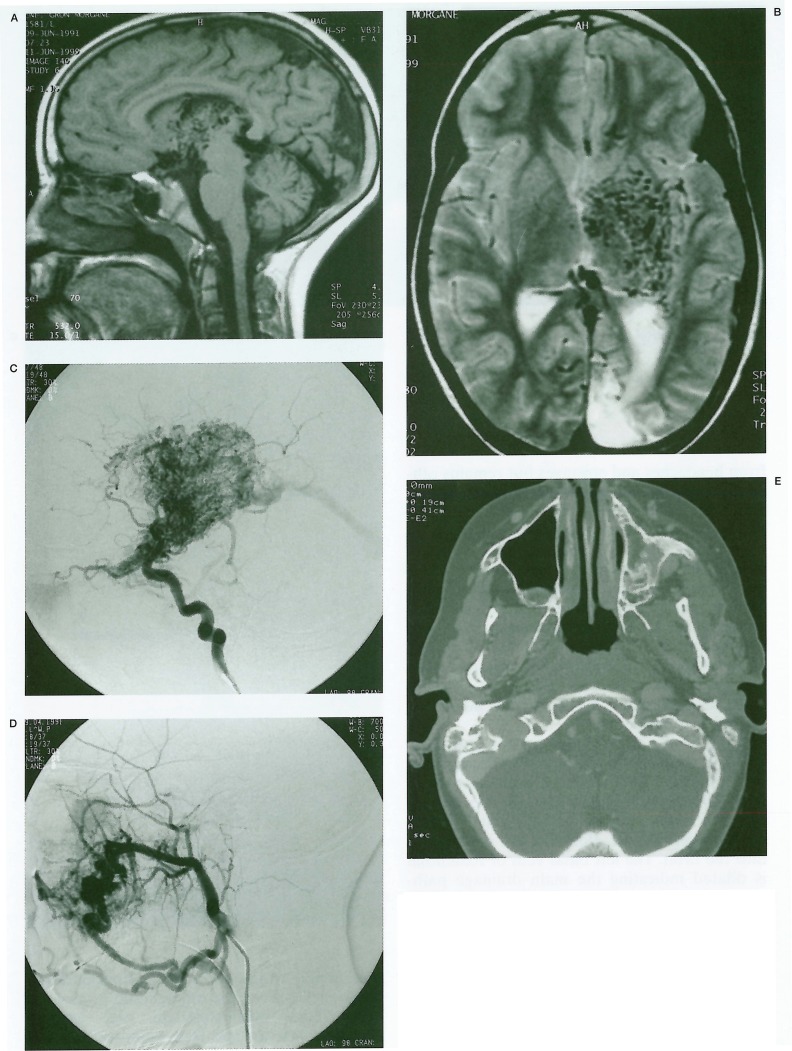
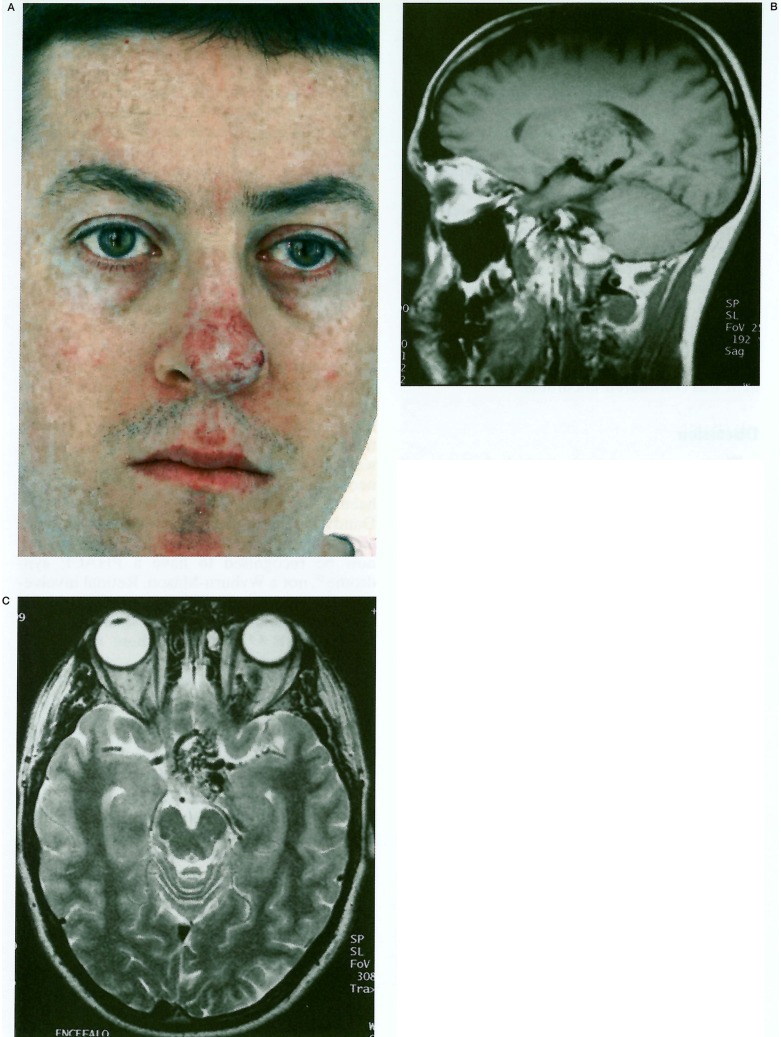
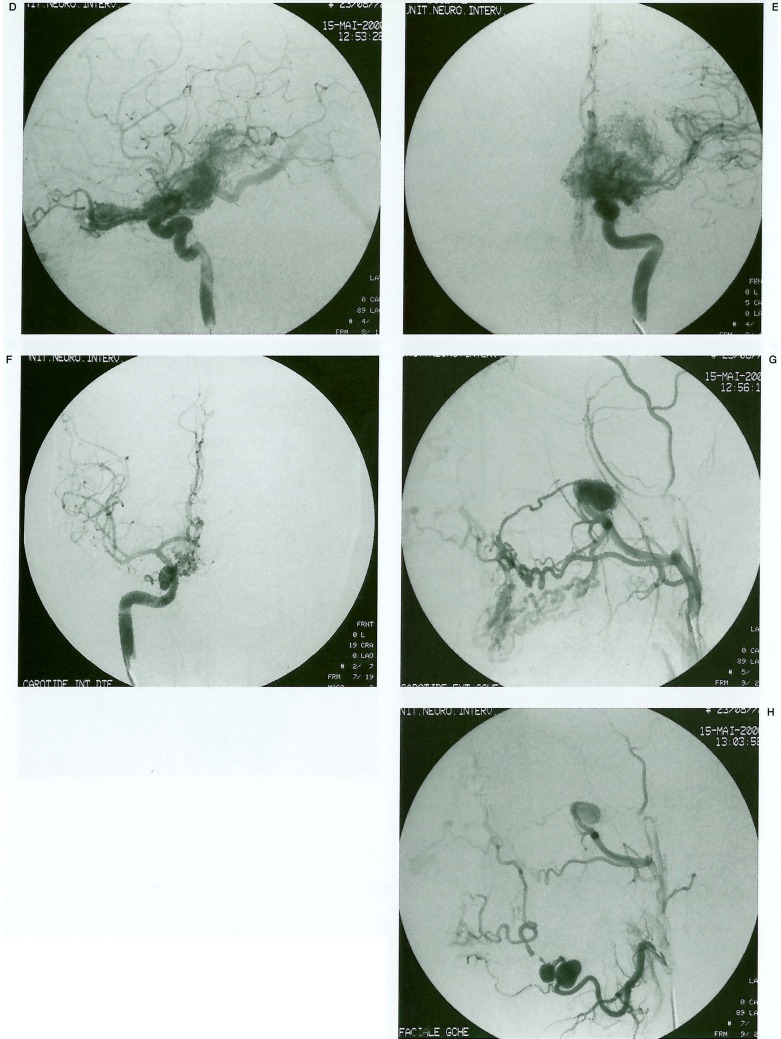
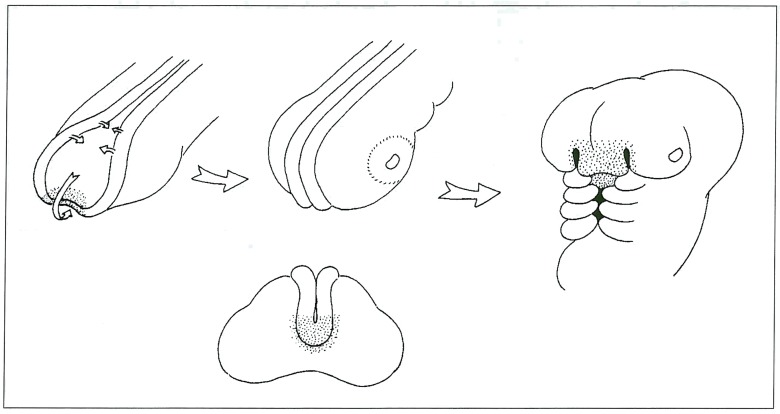
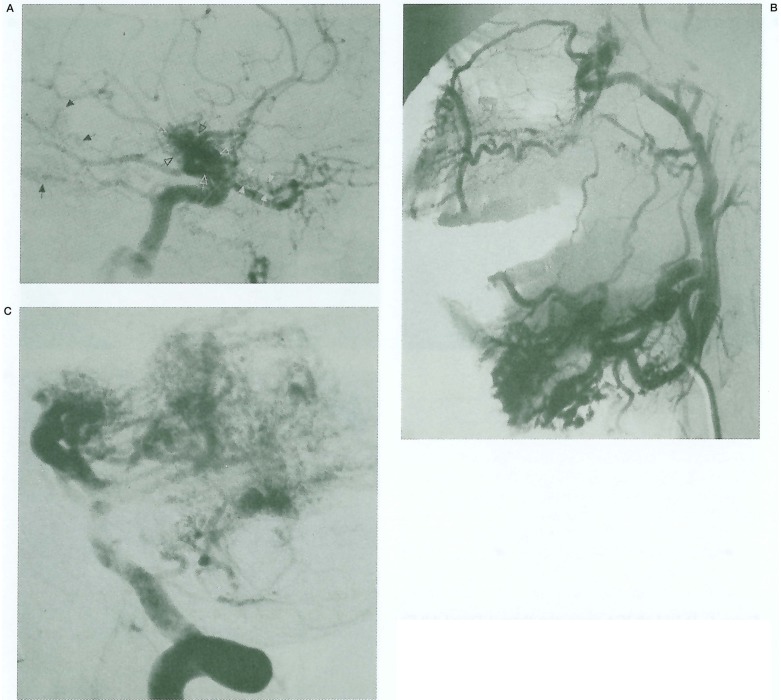
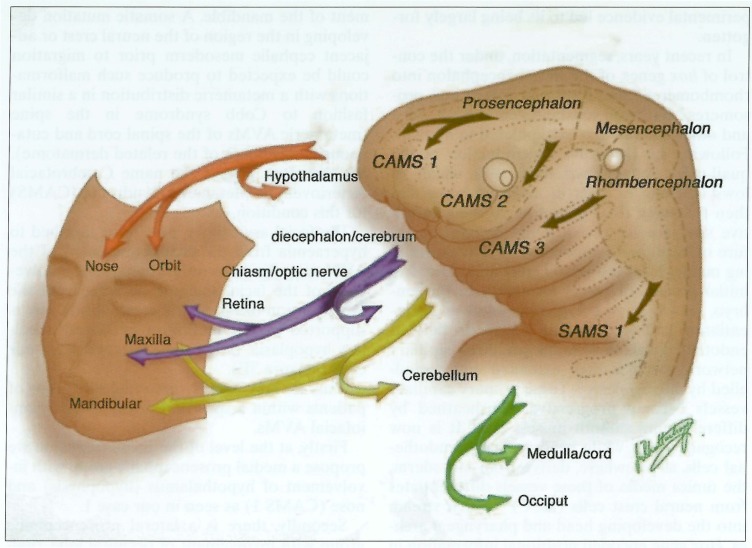
The diagnosis of Bonnet-Dechaume-Blanc or Wyburn-Mason syndrome encompasses a spectrum of phenotypic expression. Features of the syndrome as originally described, and common to all, include arteriovenous malformations of the brain and orbit (with retinal and/or retrobulbar lesions). A portion of these patients manifest the complete expression of the disease with additional high-flow arteriovenous malformations of the maxillofacial or mandibular regions. These present the distinct and additional risks of lifethreatening epistaxis or gingival haemorrhage. We suggest new diagnostic criteria for the syndrome. Applying insights from modern developmental biology to our series of 15 patients (the largest to date), together with a review of the literature, we have recognised metameric patterns of involvement in what we believe to be a disease of the neural crest or adjacent cephalic mesoderm. This allows us to propose a new rational classification reflecting the putative, underlying disorder and to suggest a new name: Cerebrofacial Arteriovenous Metameric Syndrome (CAMS).
Figures
Similar articles
-
Clinical course and angioarchitecture of cerebrofacial arteriovenous metameric syndromes. Three demonstrative cases and literature review.Interv Neuroradiol. 2002 Sep 30;8(3):251-64. doi: 10.1177/159101990200800305. Epub 2004 Oct 20. Interv Neuroradiol. 2002. PMID: 20594483 Free PMC article.
-
The congenital unilateral retinocephalic vascular malformation syndrome (bonnet-dechaume-blanc syndrome or wyburn-mason syndrome): review of the literature.Surv Ophthalmol. 2008 May-Jun;53(3):227-49. doi: 10.1016/j.survophthal.2007.10.001. Surv Ophthalmol. 2008. PMID: 18501269 Review.
-
Wyburn-Mason Syndrome.2023 Jun 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Jun 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 29630270 Free Books & Documents.
-
Cerebrofacial vascular metameric syndrome is caused by somatic pathogenic variants in PIK3CA.Cold Spring Harb Mol Case Stud. 2021 Dec 9;7(6):a006147. doi: 10.1101/mcs.a006147. Print 2021 Dec. Cold Spring Harb Mol Case Stud. 2021. PMID: 34887309 Free PMC article.
-
[Congenital retinocephalic facial vascular malformation syndrome. Bonnet-Dechaume-Blanc syndrome or Wyburn-Mason syndrome].Ophthalmologe. 2009 Jan;106(1):61-8; quiz 69. doi: 10.1007/s00347-008-1893-x. Ophthalmologe. 2009. PMID: 19159963 Review. German.
Cited by
-
Endovascular Treatment of AVMs in Glasgow.Interv Neuroradiol. 2005 Oct 5;11(Suppl 1):73-80. doi: 10.1177/15910199050110S112. Epub 2005 Oct 27. Interv Neuroradiol. 2005. PMID: 20584463 Free PMC article. No abstract available.
-
CNS imaging findings associated with Parry-Romberg syndrome and en coup de sabre: correlation to dermatologic and neurologic abnormalities.Neuroradiology. 2015 Jan;57(1):21-34. doi: 10.1007/s00234-014-1448-6. Epub 2014 Oct 11. Neuroradiology. 2015. PMID: 25304124
-
CT and MRI of congenital nasal lesions in syndromic conditions.Pediatr Radiol. 2015 Jul;45(7):1056-65. doi: 10.1007/s00247-014-3239-y. Epub 2015 Jan 9. Pediatr Radiol. 2015. PMID: 25573243 Review.
-
Growing dural sinus malformation with associated developmental venous anomaly, multiple cavernomas and facial venous malformation in an infant. An associated disease or a disease spectrum?Interv Neuroradiol. 2002 Dec 22;8(4):421-30. doi: 10.1177/159101990200800412. Epub 2004 Oct 20. Interv Neuroradiol. 2002. PMID: 20594504 Free PMC article.
-
Clinical course and angioarchitecture of cerebrofacial arteriovenous metameric syndromes. Three demonstrative cases and literature review.Interv Neuroradiol. 2002 Sep 30;8(3):251-64. doi: 10.1177/159101990200800305. Epub 2004 Oct 20. Interv Neuroradiol. 2002. PMID: 20594483 Free PMC article.
References
-
- Magnus H. Aneurysma arteriovenosum retinale. Arch Path Anat. 1874;60:38.
-
- Yates AG, Paine CG. Case of arteriovenous aneurysm within brain. Brain. 1930;53:38–46.
-
- Bonnet P, Dechaume J, Blanc E. L’anevrisme cirsoide de la retine. (Anevrisme racemeux) Ses relations avec ľanevrysme cirsoide du cerveau. Le Journal Medical de Lyon. 1937;18:165–178.
-
- Wyburn-Mason R. Arteriovenous aneurysm of midbrain and retina, facial naevi and mental changes. Brain. 1943;66:163–203.
-
- Willinsky RA, Lasjaunias P, et al. Multiple cerebral arteriovenous malformations (AVMs): Review of our experience from 203 patients with cerebral vascular lesions. Neuroradiology. 1990;32:207–210. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
