

Cost-effectiveness of computed tomographic colonography screening for colorectal cancer in the medicare population
- PMID: 20664028
- PMCID: PMC2923219
- DOI: 10.1093/jnci/djq242
Cost-effectiveness of computed tomographic colonography screening for colorectal cancer in the medicare population
Abstract
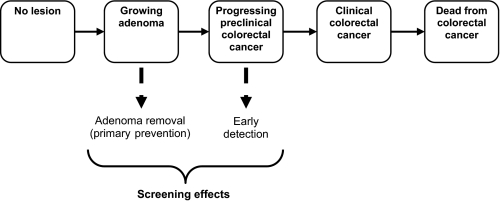
Background: The Centers for Medicare and Medicaid Services (CMS) considered whether to reimburse computed tomographic colonography (CTC) for colorectal cancer screening of Medicare enrollees. To help inform its decision, we evaluated the reimbursement rate at which CTC screening could be cost-effective compared with the colorectal cancer screening tests that are currently reimbursed by CMS and are included in most colorectal cancer screening guidelines, namely annual fecal occult blood test (FOBT), flexible sigmoidoscopy every 5 years, flexible sigmoidoscopy every 5 years in conjunction with annual FOBT, and colonoscopy every 10 years.
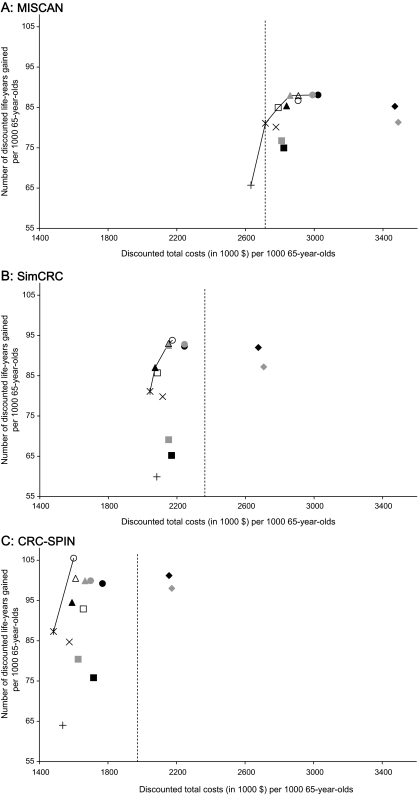
Methods: We used three independently developed microsimulation models to assess the health outcomes and costs associated with CTC screening and with currently reimbursed colorectal cancer screening tests among the average-risk Medicare population. We assumed that CTC was performed every 5 years (using test characteristics from either a Department of Defense CTC study or the National CTC Trial) and that individuals with findings of 6 mm or larger were referred to colonoscopy. We computed incremental cost-effectiveness ratios for the currently reimbursed screening tests and calculated the maximum cost per scan (ie, the threshold cost) for the CTC strategy to lie on the efficient frontier. Sensitivity analyses were performed on key parameters and assumptions.
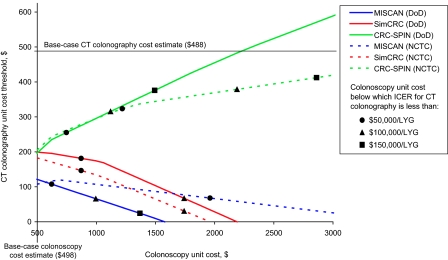
Results: Assuming perfect adherence with all tests, the undiscounted number life-years gained from CTC screening ranged from 143 to 178 per 1000 65-year-olds, which was slightly less than the number of life-years gained from 10-yearly colonoscopy (152-185 per 1000 65-year-olds) and comparable to that from 5-yearly sigmoidoscopy with annual FOBT (149-177 per 1000 65-year-olds). If CTC screening was reimbursed at $488 per scan (slightly less than the reimbursement for a colonoscopy without polypectomy), it would be the most costly strategy. CTC screening could be cost-effective at $108-$205 per scan, depending on the microsimulation model used. Sensitivity analyses showed that if relative adherence to CTC screening was 25% higher than adherence to other tests, it could be cost-effective if reimbursed at $488 per scan.
Conclusions: CTC could be a cost-effective option for colorectal cancer screening among Medicare enrollees if the reimbursement rate per scan is substantially less than that for colonoscopy or if a large proportion of otherwise unscreened persons were to undergo screening by CTC.
Figures
Comment in
-
Speaking for the evidence: colonoscopy vs computed tomographic colonography.J Natl Cancer Inst. 2010 Aug 18;102(16):1212-4. doi: 10.1093/jnci/djq286. Epub 2010 Jul 22. J Natl Cancer Inst. 2010. PMID: 20651321 No abstract available.
-
Re: Cost-effectiveness of computed tomographic colonography screening for colorectal cancer in the Medicare population.J Natl Cancer Inst. 2010 Nov 3;102(21):1676; author reply 1676-7. doi: 10.1093/jnci/djq381. Epub 2010 Sep 27. J Natl Cancer Inst. 2010. PMID: 20876419 Free PMC article. No abstract available.
References
-
- Sosna J, Morrin MM, Kruskal JB, et al. CT colonography of colorectal polyps: a metaanalysis. AJR Am J Roentgenol. 2003;181(6):1593–1598. - PubMed
-
- van Dam J, Cotton P, Johnson CD, et al. AGA future trends report: CT colonography. Gastroenterology. 2004;127(3):970–984. - PubMed
-
- Pickhardt PJ, Choi JR, Hwang I, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med. 2003;349(23):2191–2200. - PubMed
-
- Rosman AS, Korsten MA. Meta-analysis comparing CT colonography, air contrast barium enema, and colonoscopy. Am J Med. 2007;120(3):203–210. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
