

The NANETS consensus guidelines for the diagnosis and management of poorly differentiated (high-grade) extrapulmonary neuroendocrine carcinomas
- PMID: 20664477
- PMCID: PMC3100733
- DOI: 10.1097/MPA.0b013e3181ebb56f
The NANETS consensus guidelines for the diagnosis and management of poorly differentiated (high-grade) extrapulmonary neuroendocrine carcinomas
Abstract
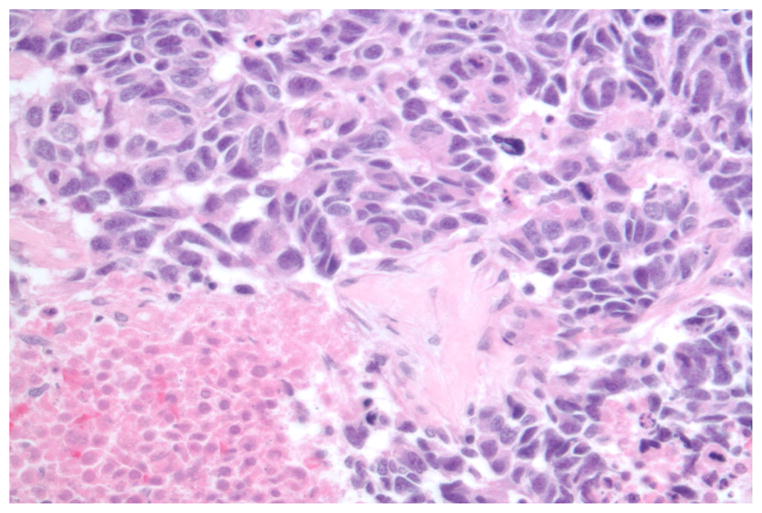
Extrapulmonary poorly differentiated neuroendocrine carcinomas can originate in the gastrointestinal tract, bladder, cervix, and prostate. These high-grade malignancies are characterized by aggressive histological features (high mitotic rate, extensive necrosis, and nuclear atypia) and a poor clinical prognosis. They are infrequently associated with secretory hormonal syndromes (such as the carcinoid syndrome) and rarely express somatostatin receptors.Most poorly differentiated neuroendocrine carcinomas are locally advanced or metastatic at presentation. First-line systemic chemotherapy with a platinum agent (cisplatin or carboplatin) and etoposide is recommended for most patients with metastatic-stage disease; however, response durations are often short. Sequential or concurrent chemoradiation is recommended for patients with loco-regional disease. In patients with localized tumors undergoing surgical resection, adjuvant treatment (chemotherapy with or without radiation) is warranted in most cases.
Figures
References
-
- Kloppel G, Heitz PU, Capella C, et al. Pathology and nomenclature of human gastrointestinal neuroendocrine (carcinoid) tumors and related lesions. World J Surg. 1996;20(2):132–141. - PubMed
-
- Capella C, Heitz PU, Hofler H, et al. Revised classification of neuroendocrine tumours of the lung, pancreas and gut. Virchows Arch. 1995;425(6):547–560. - PubMed
-
- Strosberg J, Nasir A, Coppola D, et al. Correlation between grade and prognosis in metastatic gastroenteropancreatic neuroendocrine tumors. Hum Pathol. 2009;40(9):1262–1268. - PubMed
-
-
Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: SEER 17 Regs Nov 2006 sub (1973–2004), (ed released April 2006), National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistic Branch. 2006.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
