

In the absence of renal disease, 20 year mortality risk in type 1 diabetes is comparable to that of the general population: a report from the Pittsburgh Epidemiology of Diabetes Complications Study
- PMID: 20665208
- PMCID: PMC3057031
- DOI: 10.1007/s00125-010-1860-3
In the absence of renal disease, 20 year mortality risk in type 1 diabetes is comparable to that of the general population: a report from the Pittsburgh Epidemiology of Diabetes Complications Study
Abstract
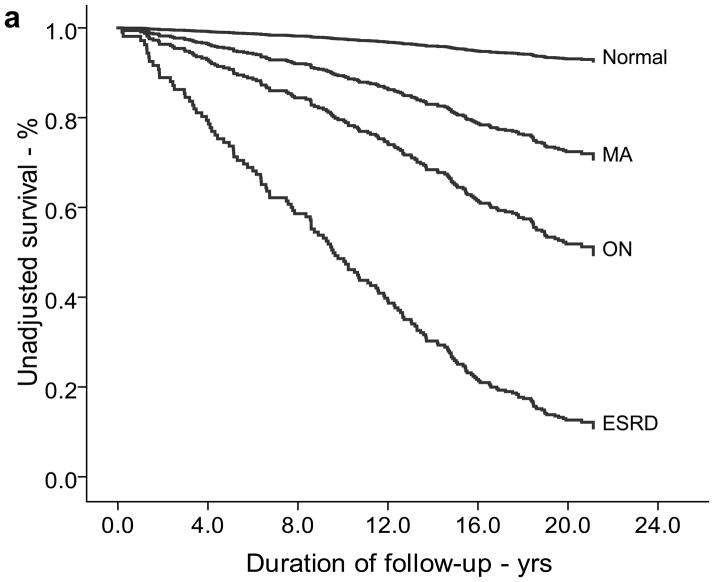
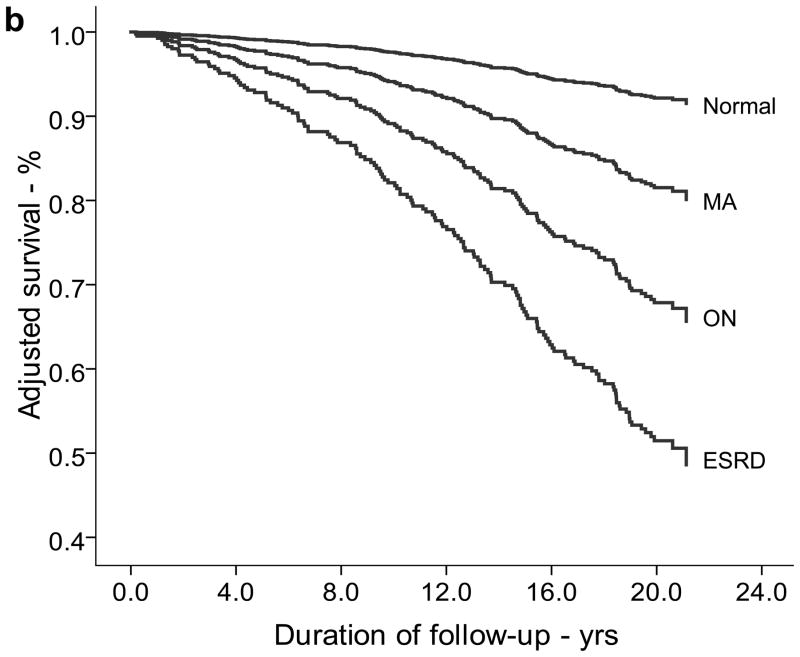
Aims/hypothesis: The FinnDiane Study has reported that mortality in type 1 diabetes is not increased over a 7 year follow-up in the absence of renal disease (RD). Using the Pittsburgh Epidemiology of Diabetes Complications (EDC) Study population (n = 658) of childhood-onset type 1 diabetes (age <17 years), the present study sought to replicate and expand these findings to a 20 year follow-up (as of 1 January 2008) and examine cause of death by renal status.
Methods: At baseline (1986-1988), mean age and duration of diabetes were 28 and 19 years, respectively. RD was defined as an albumin excretion rate ≥20 μg/min from multiple samples and grouped as microalbuminuria (MA; 20-200 μg/min), overt nephropathy (ON; >200 μg/min), or end stage renal disease (ESRD; dialysis or renal transplantation).
Results: At baseline, 311 (47.3%) individuals had RD (MA 21.3%, ON 22.2% and ESRD 3.8%). During a median 20 year follow-up, there were 152 deaths (23.1%). Mortality was 6.2 (95% CI 5.2-7.2) times higher than expected, with standardised mortality ratios of 2.0 (1.2-2.8) for normoalbuminuria (NA); 6.4 (4.4-8.4) for MA; 12.5 (9.5-15.4) for ON; and 29.8 (16.8-42.9) for ESRD. Excluding those (n = 64) with NA who later progressed to RD, no significant excess mortality was observed in the remaining NA group (1.2, 0.5-1.9), whose deaths were largely unrelated to diabetes.
Conclusions/interpretation: These data confirm the importance of RD, including persistent microalbuminuria, as a marker of mortality risk and suggest that type 1 diabetes patients without renal disease achieve long-term survival comparable to the general population.
Conflict of interest statement
We have no conflicts of interest to disclose.
Figures
References
-
- Nishimura R, LaPorte RE, Dorman JS, Tajima N, Becker D, Orchard TJ. Mortality trends in type 1 diabetes. The Allegheny County (Pennsylvania) Registry 1965–1999. Diabetes Care. 2001;24:823–827. - PubMed
-
- Messent JW, Elliott TG, Hill RD, Jarrett RJ, Keen H, Viberti GC. Prognostic significance of microalbuminuria in insulin-dependent diabetes mellitus: a twenty-three year follow-up study. Kidney Int. 1992;41:836–839. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
