

Rheumatologic manifestations of sarcoidosis
- PMID: 20665396
- PMCID: PMC3314339
- DOI: 10.1055/s-0030-1262214
Rheumatologic manifestations of sarcoidosis
Abstract
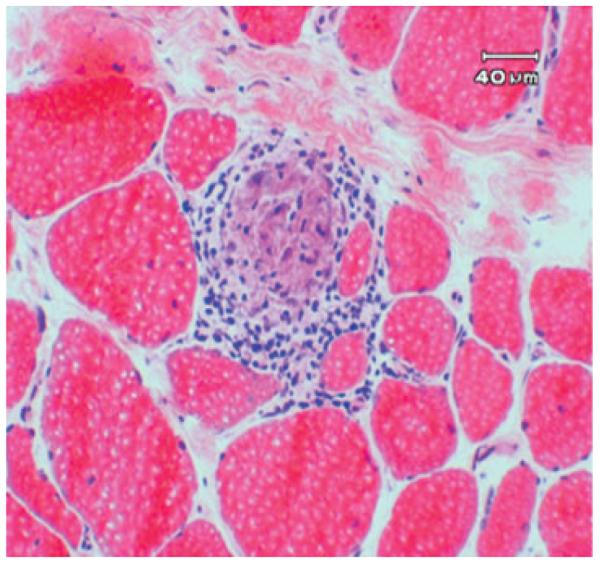
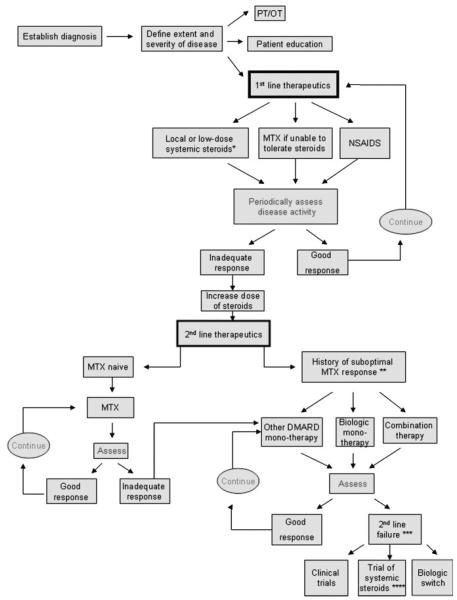
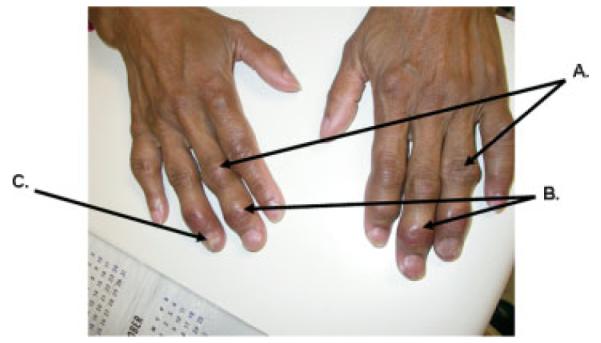
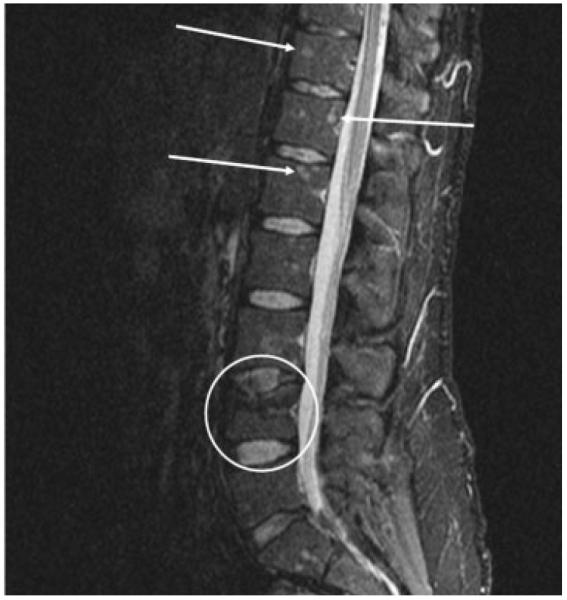
Sarcoidosis is a systemic, clinically heterogeneous disease characterized by the development of granulomas. Any organ system can be involved, and patients may present with any number of rheumatologic symptoms. There are no U.S. Food and Drug Administration-approved therapies for the treatment of sarcoidosis. Diagnosing sarcoidosis becomes challenging, particularly when its complications cause patients' symptoms to mimic other conditions, including polymyositis, Sjögren syndrome, or vasculitis. This review presents an overview of the etiology of and biomarkers associated with sarcoidosis. We then provide a detailed description of the rheumatologic manifestations of sarcoidosis and present a treatment algorithm based on current clinical evidence for patients with sarcoid arthritis. The discussion will focus on characteristic findings in patients with sarcoid arthritis, osseous involvement in sarcoidosis, and sarcoid myopathy. Arthritic conditions that sometimes coexist with sarcoidosis are described as well. We present two cases of sarcoidosis with rheumatologic manifestations. Our intent is to encourage a multidisciplinary, translational approach to meet the challenges and difficulties in understanding and treating sarcoidosis.
Copyright Thieme Medical Publishers.
Figures


References
-
- Hofmann S, Franke A, Fischer A, et al. Genome-wide association study identifies ANXA11 as a new susceptibility locus for sarcoidosis. Nat Genet. 2008;40:1103–1106. - PubMed
-
- Chen ES, Moller DR. Etiology of sarcoidosis. Clin Chest Med. 2008;29:365–377. vii. - PubMed
-
- Smith G, Brownell I, Sanchez M, Prystowsky S. Advances in the genetics of sarcoidosis. Clin Genet. 2008;73:401–412. - PubMed
-
- Drake WP, Newman LS. Mycobacterial antigens may be important in sarcoidosis pathogenesis. Curr Opin Pulm Med. 2006;12:359–363. - PubMed
-
- Ezzie ME, Crouser ED. Considering an infectious etiology of sarcoidosis. Clin Dermatol. 2007;25:259–266. - PubMed
