

Use of white blood cell growth factors and risk of acute myeloid leukemia or myelodysplastic syndrome among elderly patients with non-Hodgkin lymphoma
- PMID: 20665502
- PMCID: PMC6300149
- DOI: 10.1002/cncr.25525
Use of white blood cell growth factors and risk of acute myeloid leukemia or myelodysplastic syndrome among elderly patients with non-Hodgkin lymphoma
Abstract
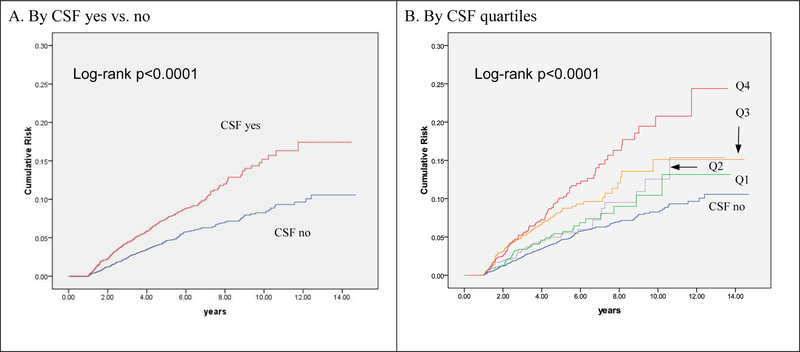
Background: The current study was conducted to evaluate the association between colony-stimulating factor (CSF) use and the risk of developing therapy-related myelodysplastic syndromes or acute myeloid leukemia (t-MDS/AML) among a large cohort of elderly patients with non-Hodgkin lymphoma (NHL) who were treated with chemotherapy.
Methods: A total of 13,203 NHL patients were identified from the Surveillance, Epidemiology, and End Results-Medicare database who were diagnosed from 1992 through 2002. Patients were followed from their initial chemotherapy date until the date they were diagnosed with t-MDS/AML, death, or last follow-up (October 31, 2006), whichever occurred first.
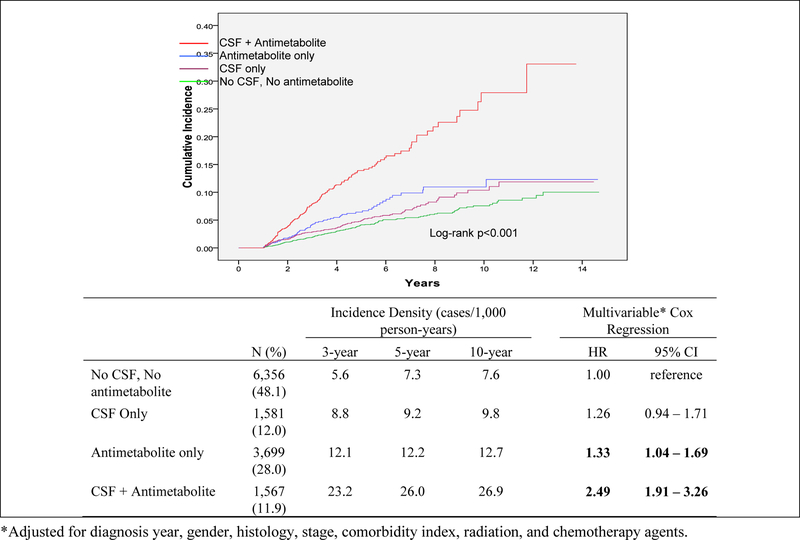
Results: Overall, 40% (n = 5266) of patients received CSF. During the follow-up period (median follow-up, 2.9 years [range, 1-14.7 years]), 272 (5.2%) patients who were treated with CSF developed t-MDS/AML, compared with 230 (2.9%) patients who did not (P < .0001, log-rank test). The 5-year incidence of t-MDS/AML for patients receiving CSF was 14.1 per 1000 person-years compared with 8.3 per 1000 person-years for patients not receiving CSF. In a multivariable Cox regression analysis adjusted for gender, histology, stage, comorbidities, radiotherapy, and chemotherapy agent, CSF use was found to be independently associated with a 53% increased risk of t-MDS/AML (hazard ratio [HR], 1.53; 95% confidence interval [95% CI], 1.26-1.84). The observed association between CSF use and t-MDS/AML persisted across histologic subgroups (ie, diffuse large B-cell lymphoma, follicular lymphoma, and others). Patients who received both CSF and antimetabolite chemotherapy were found to have a 2.5-fold increased risk of t-MDS/AML (HR, 2.49; 95% CI, 1.91-3.26) compared with patients who received neither agent.
Conclusions: The current study, which to our knowledge is the first large population-based study published to date, demonstrated that the administration of CSF among elderly NHL patients receiving chemotherapy was associated with an increased risk of t-MDS/AML, although the absolute risk was low.
Copyright © 2010 American Cancer Society.
Figures
References
-
- Vega-Stromberg T Chemotherapy-induced secondary malignancies. J Infus Nurs 2003;26:353–61. - PubMed
-
- Godley L, Larson R. The syndrome of therapy-related myelodysplasia and myeloid leukemia. In: Bennett J, ed. The Myelodysplastic Syndromes: Pathology and Clinical Management Marcel Dekker, Inc, 2002:139–76.
-
- Leone G, Mele L, Pulsoni A, Equitani F, Pagano L. The incidence of secondary leukemias. Haematologica 1999;84:937–945. - PubMed
-
- Travis LB, Curtis RE, Stovall M, et al. Risk of leukemia following treatment for non-Hodgkin’s lymphoma. J Natl Cancer Inst 1994;86:1450–7. - PubMed
-
- Greene MH, Wilson J. Second cancer following lymphatic and hematopoietic cancers in Connecticut, 1935–82. Natl Cancer Inst Monogr 1985;68:191–217. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
