

Acquired angioedema
- PMID: 20667117
- PMCID: PMC2925362
- DOI: 10.1186/1710-1492-6-14
Acquired angioedema
Abstract
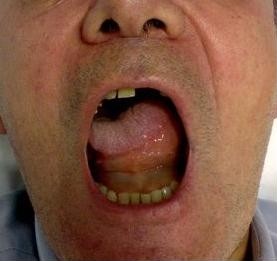
Acquired angioedema (AAE) is characterized by acquired deficiency of C1 inhibitor (C1-INH), hyperactivation of the classical pathway of human complement and angioedema symptoms mediated by bradykinin released by inappropriate activation of the contact-kinin system. Angioedema recurs at unpredictable intervals, lasts from two to five days and presents with edema of the skin (face, limbs, genitals), severe abdominal pain with edema of the gastrointestinal mucosa, life-threateing edema of the upper respiratory tract and edema of the oral mucosa and of the tongue. AAE recurs in association with various conditions and particularly with different forms of lymphoproliferative disorders. Neutralizing autoantibodies to C1-INH are present in the majority of patients. The therapeutic approach to a patient with AAE should first be aimed to avoid fatalities due to angioedema and then to avoid the disability caused be angioedema recurrences. Acute attacks can be treated with plasma-derived C1-INH, but some patients become non-responsive and in these patients the kallikrein inhibitor ecallantide and the bradykinin receptor antagonist icatibant can be effective. Angioedema prophylaxis is performed using antifibrinolytic agents and attenuated androgens with antifibrinolytic agents providing somewhat better results. Treatment of the associated disease can resolve AAE in some patients.
Figures

References
-
- Caldwell JR, Ruddy S, Schur PH, Austen KF. Acquired C1 inhibitor deficiency in lymphosarcoma. Clin Immunol Immunopathol. 1972;1:39–52. doi: 10.1016/0090-1229(72)90006-2. - DOI
-
- Agostoni A, Aygören-Pürsün E, Binkley KE, Blanch A, Bork K, Bouillet L, Bucher C, Castaldo AJ, Cicardi M, Davis AE, De Carolis C, Drouet C, Duponchel C, Farkas H, Fáy K, Fekete B, Fischer B, Fontana L, Füst G, Giacomelli R, Gröner A, Hack CE, Harmat G, Jakenfelds J, Juers M, Kalmár L, Kaposi PN, Karádi I, Kitzinger A, Kollár T. Hereditary and acquired angioedema: problems and progress: proceedings of the third C1 esterase inhibitor deficiency workshop and beyond. J Allergy Clin Immunol. 2004;114:S51–131. doi: 10.1016/j.jaci.2004.06.047. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
