

doi: 10.1186/1749-799X-5-48.
Ilizarov treatment of humeral shaft nonunion in an antiepileptic drug patient with uncontrolled generalized tonic-clonic seizure activity
Affiliations
- PMID: 20667134
- PMCID: PMC2919461
- DOI: 10.1186/1749-799X-5-48
Item in Clipboard
Ilizarov treatment of humeral shaft nonunion in an antiepileptic drug patient with uncontrolled generalized tonic-clonic seizure activity
J Orthop Surg Res.
.
Abstract
Nonunion of the humeral shaft in patients with antiepileptic drug associated metabolic bone disorder constitute a challenging surgical problem difficult to treat due to seizure activity, osteoporosis, and poor stabilization options. We report a case of nonunion of the humeral shaft in an antiepileptic drug patient with uncontrolled generalized tonic-clonic seizure activity successfully treated with Ilizarov external fixator and a follow-up of 4 years.
Figures
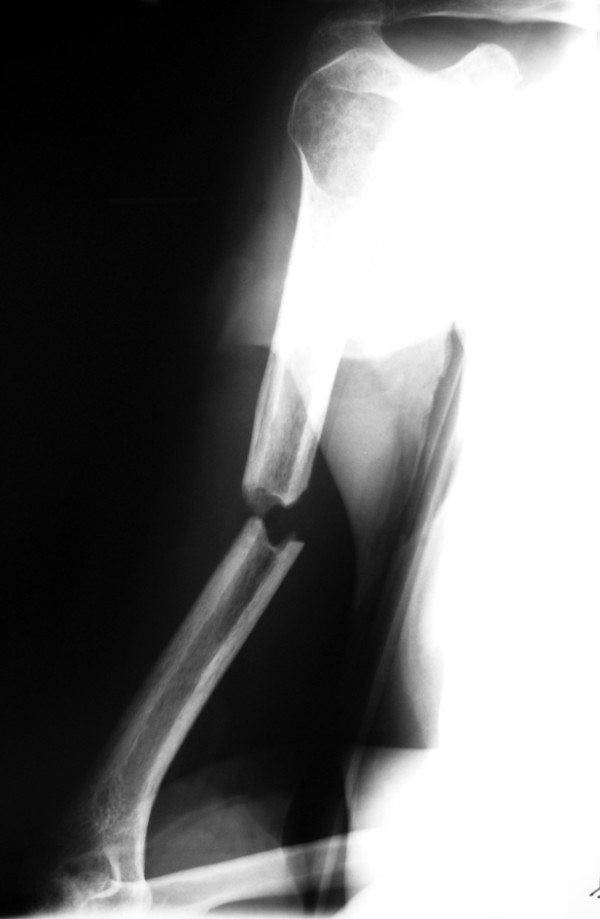
Anteroposteriorradiograph of the right humerus of a 43-year-old man sustained a transverse diaphyseal fracture after a fall during a generalized tonic-clonic attack.

Lateral view of the right humerus.
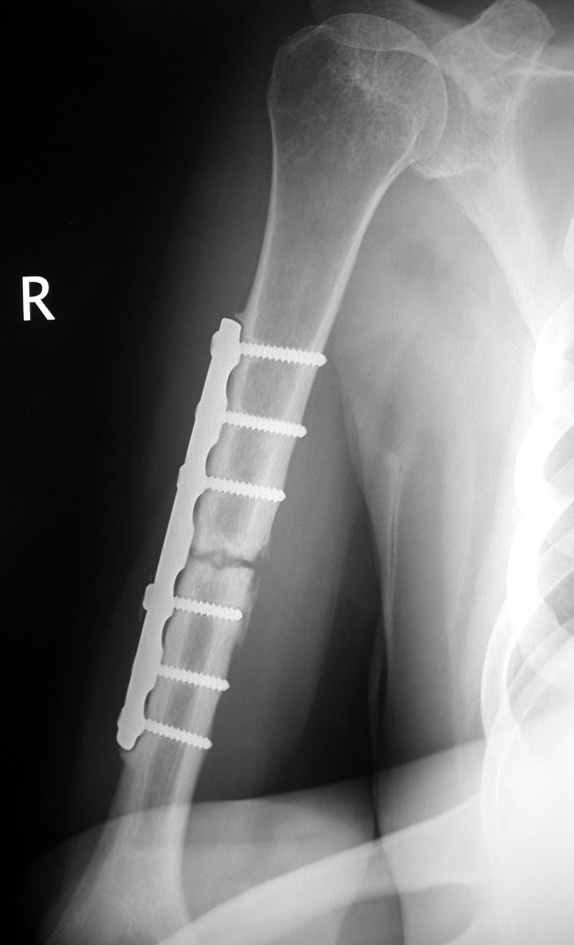
Anteroposteriorradiograph of the right humerus showing atrophic nonunion of the humeral shaft 18 months after treatment with open reduction and internal fixation.
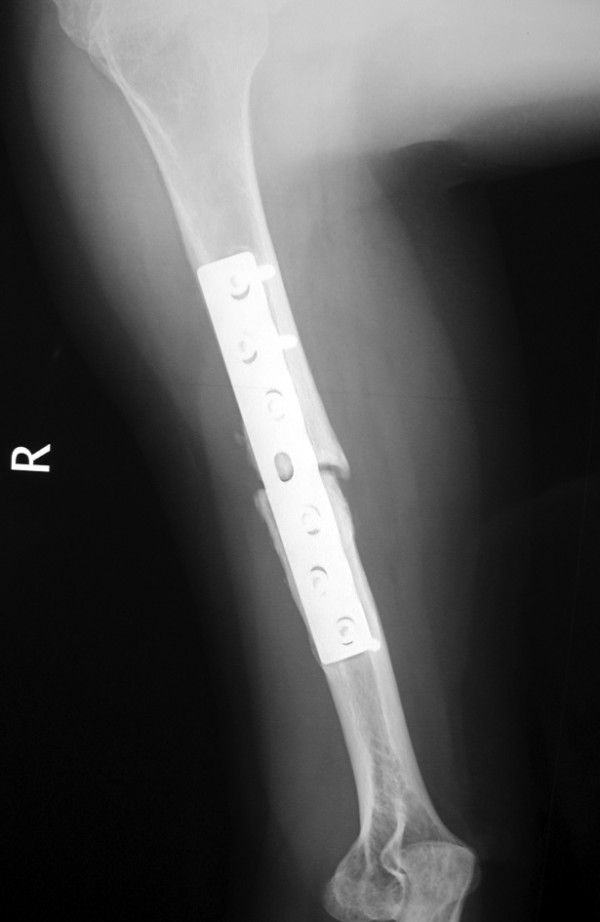
Lateral view of the right humerus 18 months postoperatively.

Radiograph of the3-ring frame.

Photograph of the same Ilizarov circular frame. Note the proximal and distal 5/8 rings that facilitate active shoulder and elbow range of motion.
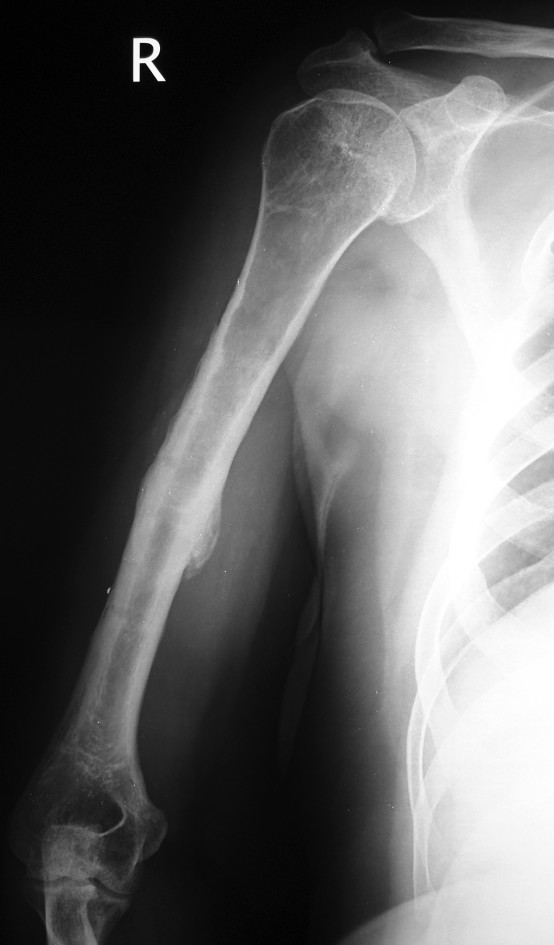
Anteroposteriorradiograph of the humeral fracture 4 years after surgery. Union was achieved 4.5 months after initial application of the frame.

Lateral view of the humeral fracture 4 years postoperatively.
Similar articles
-
Treatment of the humeral shaft aseptic nonunion using plate or unilateral external fixator.J Trauma. 2008 May;64(5):1290-6. doi: 10.1097/TA.0b013e3180582471. J Trauma. 2008. PMID: 18469652
-
Treatment of the humeral shaft nonunion after surgical failure using the Selfdynamisable internal fixator.Arch Orthop Trauma Surg. 2007 Oct;127(8):713-8. doi: 10.1007/s00402-007-0331-x. Epub 2007 Apr 25. Arch Orthop Trauma Surg. 2007. PMID: 17457596
-
Lamotrigine adjunctive therapy among children and adolescents with primary generalized tonic-clonic seizures.Pediatrics. 2006 Aug;118(2):e371-8. doi: 10.1542/peds.2006-0148. Epub 2006 Jul 17. Pediatrics. 2006. PMID: 16847080 Clinical Trial.
-
Nonunion of the humerus following intramedullary nailing treated by Ilizarov hybrid fixation.J Orthop Trauma. 1998 Feb;12(2):138-41. doi: 10.1097/00005131-199802000-00013. J Orthop Trauma. 1998. PMID: 9503305
-
[First generalized tonic-clonic seizure].Tidsskr Nor Laegeforen. 2015 Aug 11;135(14):1256-8. doi: 10.4045/tidsskr.14.0654. eCollection 2015 Aug 11. Tidsskr Nor Laegeforen. 2015. PMID: 26269067 Review. Norwegian.
References
-
- Brinker MR, O'Connor DP. The incidence of fractures and dislocations referred for orthopaedic services in a capitated population. J Bone Joint Surg Am. 2004;86:290–7. - PubMed
-
- Healy WL, White GM, Mick CA, Brooker AF Jr, Weiland AJ. Nonunion of the humeral shaft. Clin Orthop Rel Res. 1987;219:206–13. - PubMed
LinkOut - more resources
Full Text Sources
