

Midterm outcome of partially thrombosed intracranial aneurysms treated with guglielmi detachable coils
- PMID: 20667178
- PMCID: PMC3679574
- DOI: 10.1177/159101990000600103
Midterm outcome of partially thrombosed intracranial aneurysms treated with guglielmi detachable coils
Abstract
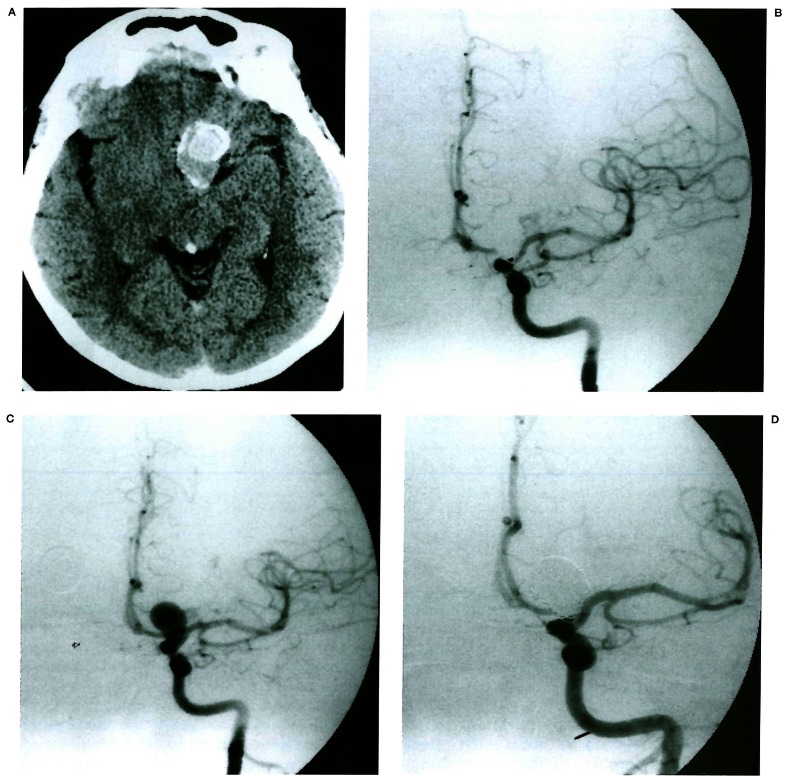
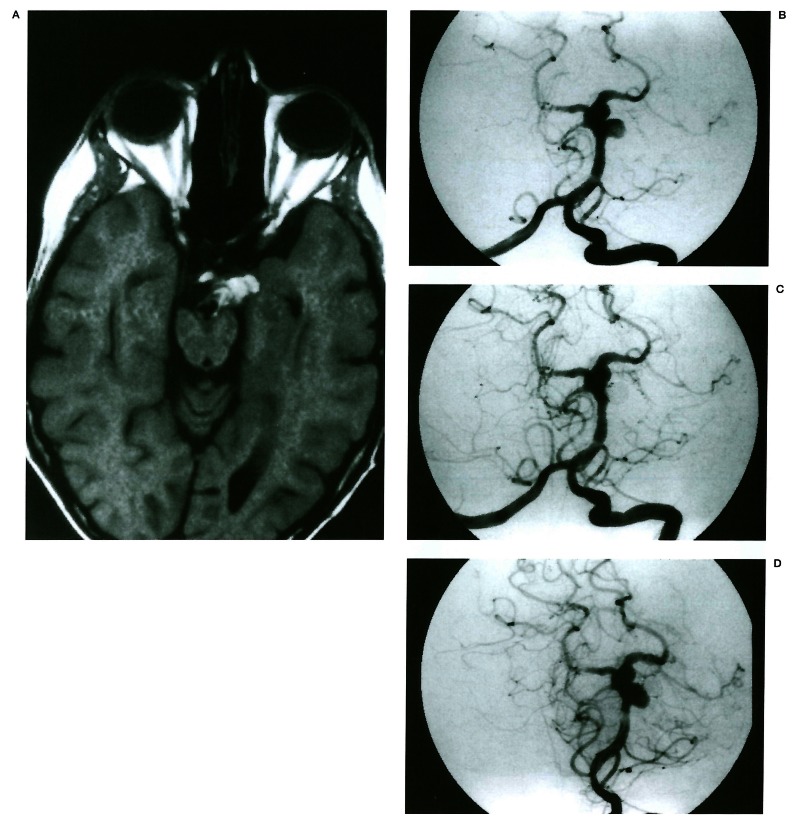
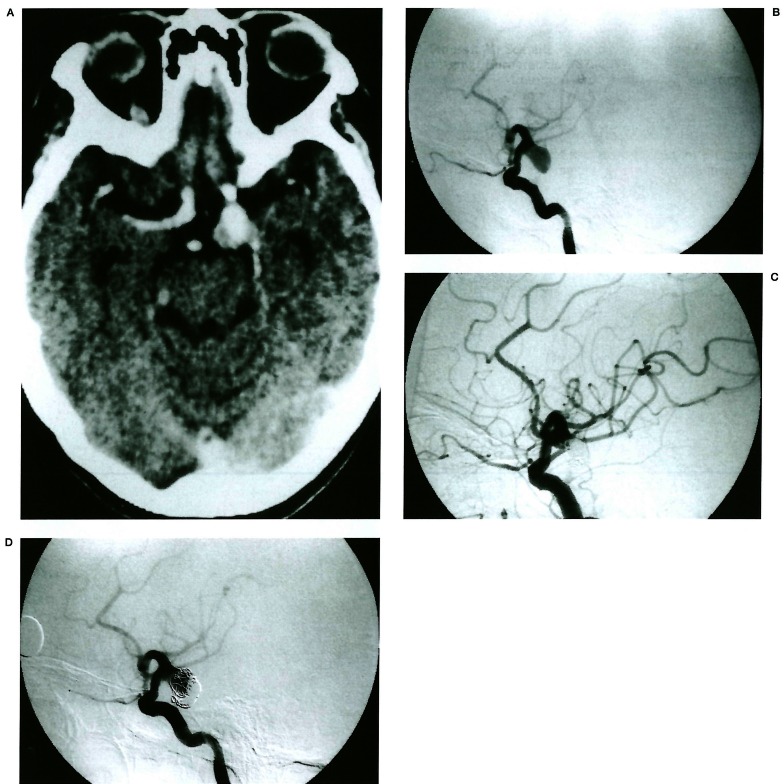
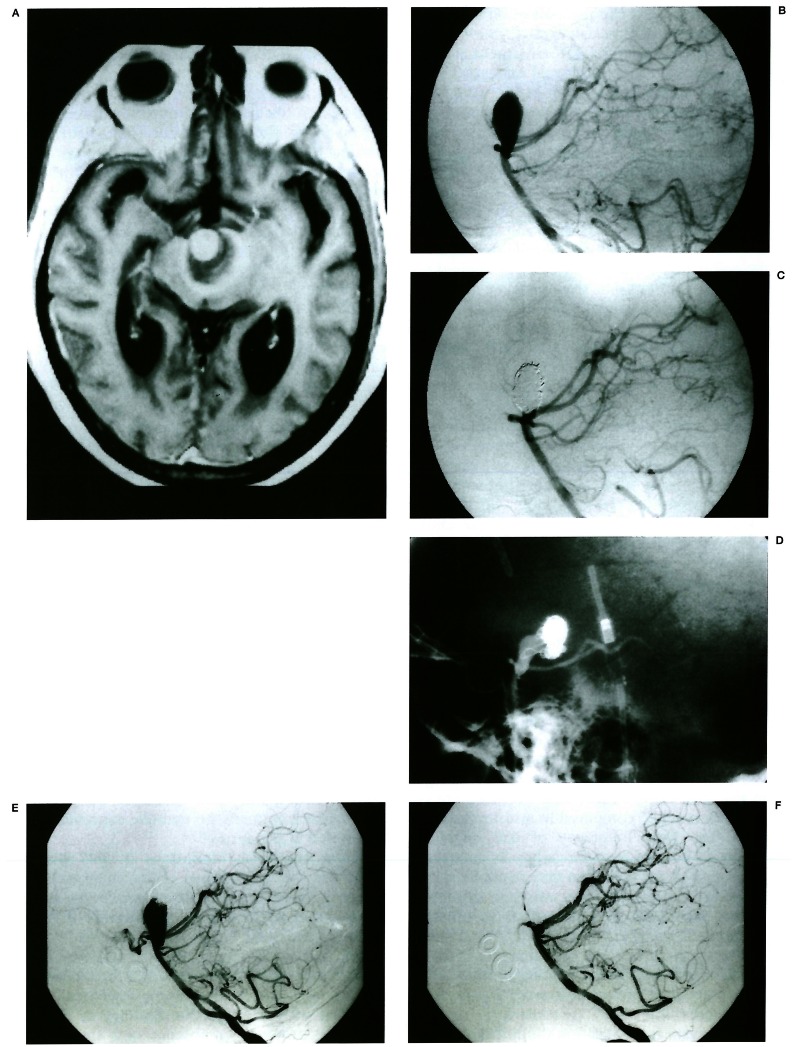
We evaluated the results of Guglielmi detachable coil (GDC) treatment in partially thrombosed aneurysms and determined if there is high rate of recanalisation on follow-up. Among 149 treated aneurysms in 141 patients, 25 CT- or MR-confirmed partially thrombosed aneurysms were selected for evaluation. The features of thrombosed aneurysms and percentage of occlusion were analysed on initial angiograms. Follow-up angiograms, which were available in 18 cases, were evaluated for aneurysm lumen recanalisation. The recanalisation rate was compared with that of non-thrombosed aneurysms treated with GDCs. Locations of aneurysms were as follows: cavernous carotid ten; ophthalmic four; p-com. two; MCA one; A-com. one; basilar tip four; midbasilar two; PICA one. The size of the aneurysm lumen ranged from 5 to 30 mm (mean 16.8 mm) on angiograms, but on cross sectional images the size of aneurysms ranged from 13 to 70 mm (mean 24.6 mm). The extent of aneurysmal thrombosis ranged from 10 to 90 per cent (mean 46.4 per cent). On initial GDC treatment, total to subtotal occlusion was achieved in 18 cases out of 25 (72%). Of the 18 follow-up angiograms, 14 cases (77.8%) showed recanalisation ranging from 10 to 60 per cent of aneurysm size. Luminal recanalisation was due to migration (10 of 14) or compaction (4 of 14) of coil masses. In two cases, symptoms recurred in association with aneurysm recanalisation, but in no instance was haemorrhage noted. Attempts for retreatment were made in ten cases with success in six. In comparison, 14 (15.9%) out of 88 nonthrombosed cases revealed recanalisation on follow-up angiography. Midterm follow-up angiograms in partially thrombosed aneurysms treated with GDC revealed a fivefold higher rate of recanalisation than in non-thrombosed cases. Close follow-up is necessary in patients with thrombosed aneurysms treated with GDCs.
Figures
Similar articles
-
GDC Embolisation of Cavernous Internal Carotid Artery Aneurysms with Parent Artery Preservation.Interv Neuroradiol. 2000 Dec 22;6(4):291-8. doi: 10.1177/159101990000600403. Epub 2001 May 15. Interv Neuroradiol. 2000. PMID: 20667207 Free PMC article.
-
Treatment of basilar artery bifurcation aneurysms by using Guglielmi detachable coils: a 6-year experience.J Neurosurg. 1999 May;90(5):843-52. doi: 10.3171/jns.1999.90.5.0843. J Neurosurg. 1999. PMID: 10223449
-
Efficacy and current limitations of intravascular stents for intracranial internal carotid, vertebral, and basilar artery aneurysms.J Neurosurg. 1999 Oct;91(4):538-46. doi: 10.3171/jns.1999.91.4.0538. J Neurosurg. 1999. PMID: 10507372
-
Selection of cerebral aneurysms for treatment using Guglielmi detachable coils: the preliminary University of Illinois at Chicago experience.Neurosurgery. 1998 Dec;43(6):1281-95; discussion 1296-7. doi: 10.1097/00006123-199812000-00011. Neurosurgery. 1998. PMID: 9848841 Review.
-
Follow-up angiography of intracranial aneurysms treated with endovascular placement of Guglielmi detachable coils.Neurosurgery. 2002 Feb;50(2):239-49; discussion 249-50. doi: 10.1097/00006123-200202000-00003. Neurosurgery. 2002. PMID: 11844258 Review.
Cited by
-
Endovascular treatment of giant or very large intracranial aneurysms with different modalities: an analysis of 20 cases.Neuroradiology. 2007 Oct;49(10):819-28. doi: 10.1007/s00234-007-0257-6. Epub 2007 Jul 5. Neuroradiology. 2007. PMID: 17611747
-
Additional coiling of previously coiled cerebral aneurysms: clinical and angiographic results.AJNR Am J Neuroradiol. 2004 Sep;25(8):1373-6. AJNR Am J Neuroradiol. 2004. PMID: 15466335 Free PMC article.
-
Woven Endobridge (WEB) Device as a Retreatment Strategy After Unsuccessful Surgical Clipping.World Neurosurg. 2020 Jul;139:111-120. doi: 10.1016/j.wneu.2020.02.101. Epub 2020 Mar 13. World Neurosurg. 2020. PMID: 32179191 Free PMC article.
-
Endovascular Treatment of Very Large and Giant Intracranial Aneurysms: Comparison between Reconstructive and Deconstructive Techniques-A Meta-Analysis.AJNR Am J Neuroradiol. 2018 May;39(5):852-858. doi: 10.3174/ajnr.A5591. Epub 2018 Mar 15. AJNR Am J Neuroradiol. 2018. PMID: 29545248 Free PMC article.
-
Endovascular Treatment of "Donut-Shaped" Aneurysm-A Case Series.Medicina (Kaunas). 2024 Jul 9;60(7):1116. doi: 10.3390/medicina60071116. Medicina (Kaunas). 2024. PMID: 39064545 Free PMC article.
References
-
- Atkinson JLD, Lane JI, et al. Spontaneous thrombosis of posterior cerebral artery aneurysm with angiographic reappearance. J Neurosurg. 1993;79:434–437. - PubMed
-
- Housepain EM, Pool JL. A systemic analysis of intracranial aneurysms from the autopsy file of the Presbyterian Hospital. 1914-1956. J Neuropathol Exp Neurol. 1958;17:409–423. - PubMed
-
- Spallone A, Cantore G. The role of extracranial carotid abnormalities in the genesis of cerebral aneurysms. J Neurosurg. 1981;55:693–700. - PubMed
-
- Weir B, Macdonald RL. Intracranial aneurysms and subarachnoid haemorrhage: an overview. In: Wilkins RH, Rengachary SS, editors. Neurosurgery. 2nd ed. Vol. 2. New York, NY: McGraw-Hill; 1996. pp. 2191–2213.
-
- Malisch TW, Guglielmi G, et al. Intracranial aneurysms treated with the Guglielmi detachable coil: midterm clinical results in a consecutive series of 100 patients. J Neurosurg. 1997;87:176–183. - PubMed
LinkOut - more resources
Full Text Sources
