

Treatment of traumatic carotid-cavernous fistula
- PMID: 20667206
- PMCID: PMC3679701
- DOI: 10.1177/159101990000600402
Treatment of traumatic carotid-cavernous fistula
Abstract
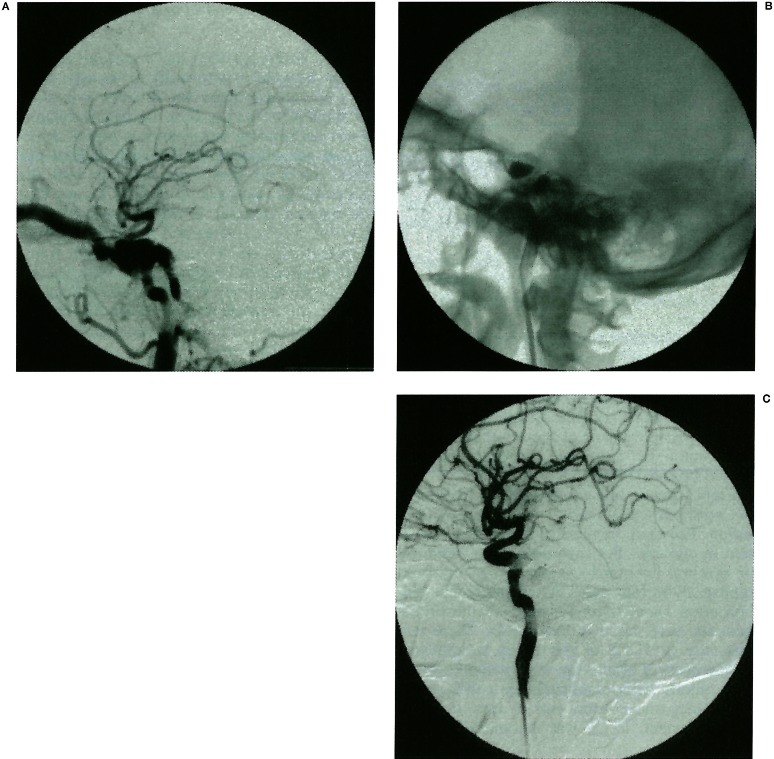
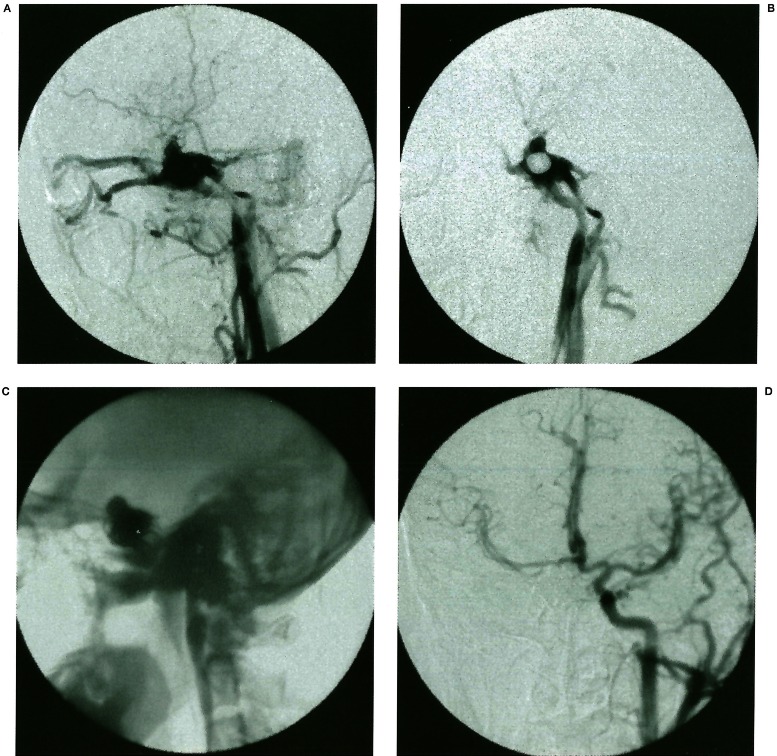
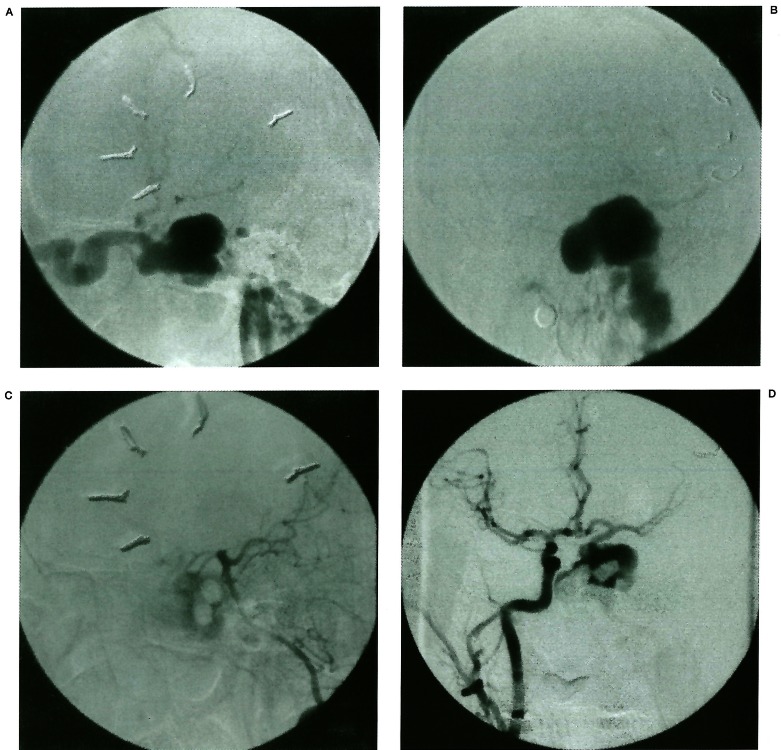
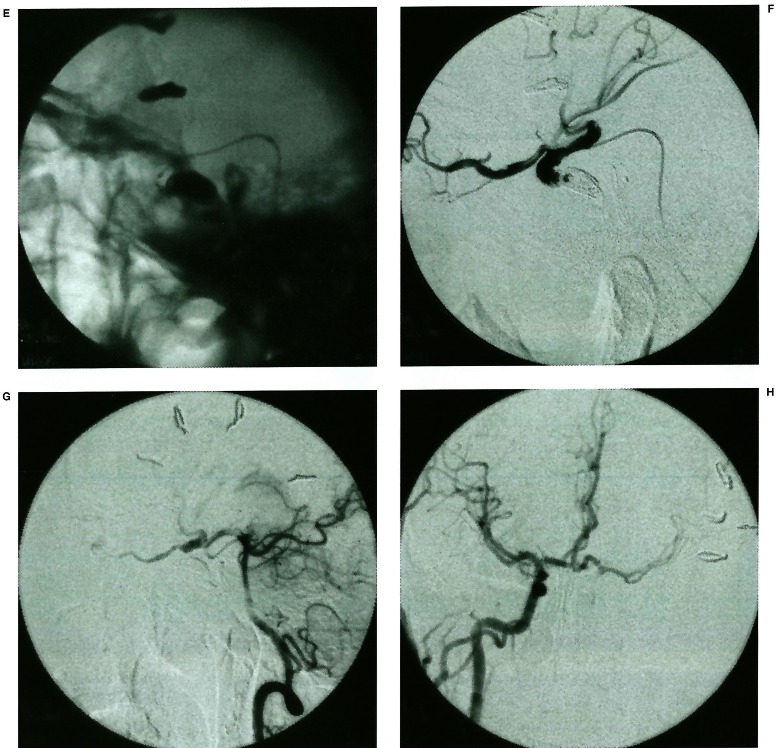
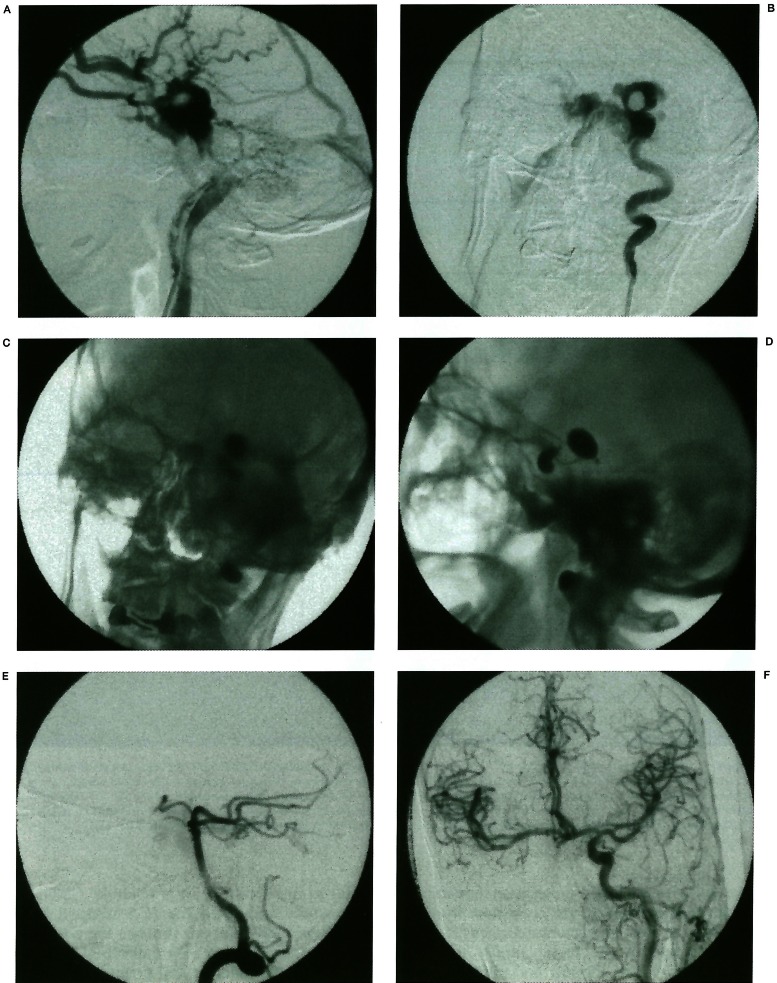
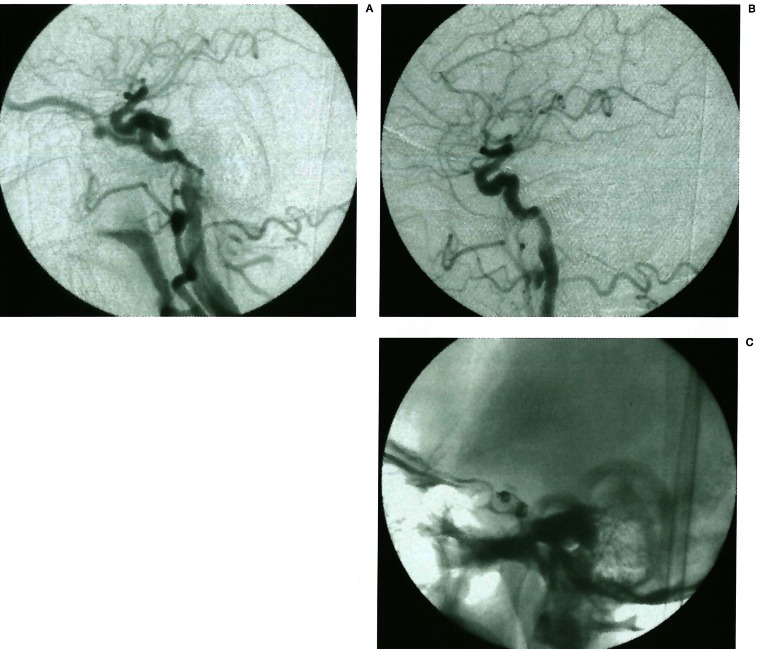
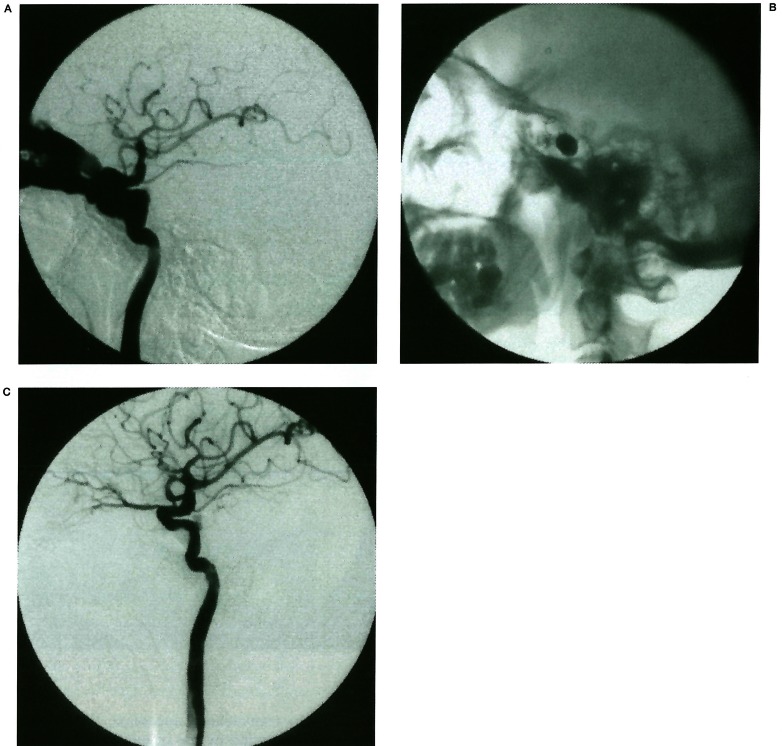
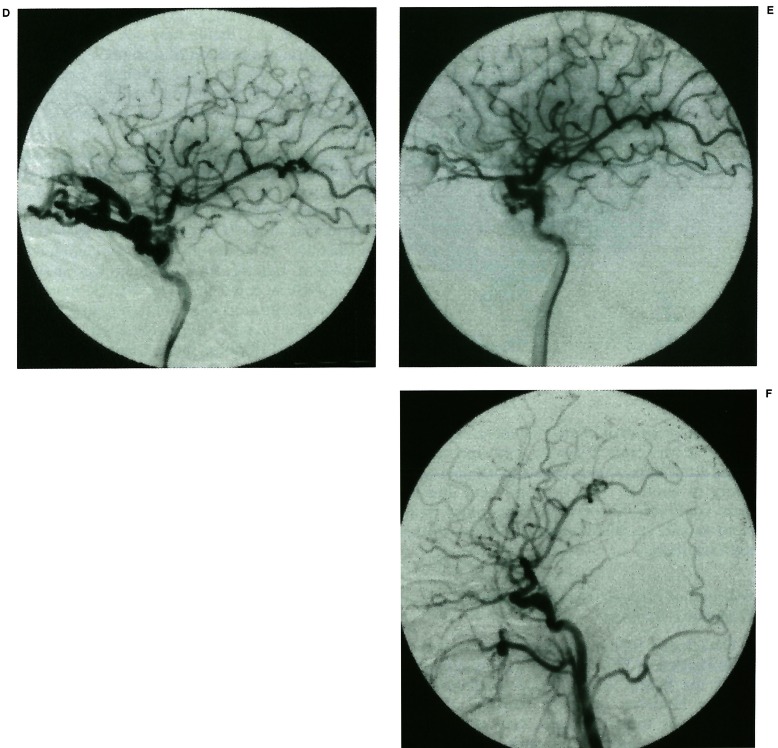
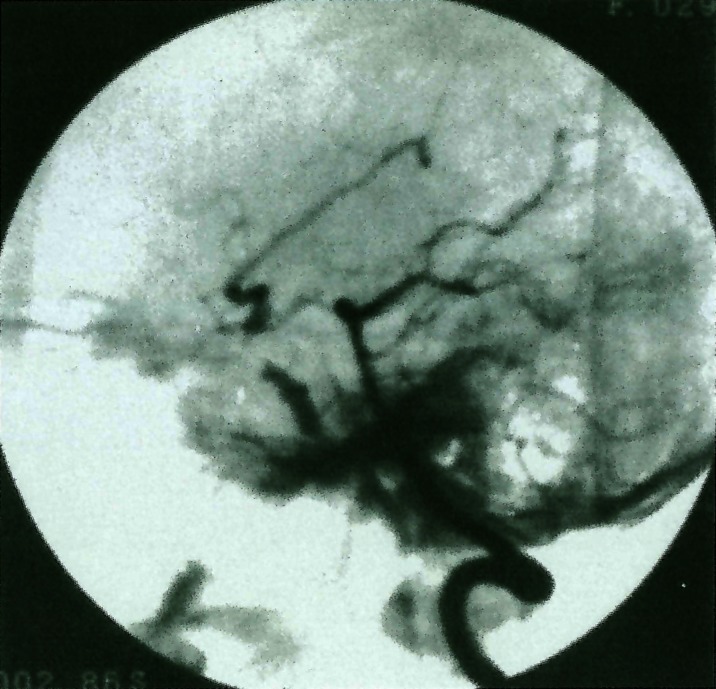
From 1986 to the end of 1998, 482 cases of traumatic carotid-cavernous fistula (TCCF) were treated by means of intravascular embolisation technique. The experience is overviewed in this article. Many kinds of detachable balloon catheters (including Chinese made detachable balloon catheters), coils and cyanoacrylate were used as embolic materials. Transcervical, transfemoral, anterior communicating artery, posterior communicating artery approach, or transvenous approach were selected according to conditions. A combination of different approaches or materials was used for complex TCCF. We found that the special sign, named "bileakage sign", indicated multileakage of TCCF and was not mentioned before.All 482 cases of TCCF were embolised successfully, of which 405 cases maintained the patency of internal carotid artery (ICA). No death related to the treatment occurred in our group and the symptoms or signs in 462 cases were relieved after embolisation. Emergency embolisation was needed in some conditions such as serious epistaxis, delayed or repeatedly subdural haematoma and rapid visual impairment. Endovascular treatment of TCCF is a safe and efficient method. The time of operation, approach, and materials for embolisation must be carefully selected in order to obtain the best result.
Figures
Similar articles
-
Endovascular embolization of traumatic carotid cavernous fistulas.Chin Med J (Engl). 1999 May;112(5):433-7. Chin Med J (Engl). 1999. PMID: 11593514
-
Bilateral traumatic carotid-cavernous fistulae: Strategies for endovascular treatment.Acta Neurochir (Wien). 2007;149(7):675-80; discussion 680. doi: 10.1007/s00701-007-1229-7. Epub 2007 Jun 11. Acta Neurochir (Wien). 2007. PMID: 17558454
-
Multimodal endovascular treatment for traumatic carotid-cavernous fistula.Chin J Traumatol. 2013;16(6):334-8. Chin J Traumatol. 2013. PMID: 24295578
-
Endovascular techniques for treatment of carotid-cavernous fistula.J Neuroophthalmol. 2009 Mar;29(1):62-71. doi: 10.1097/WNO.0b013e3181989fc0. J Neuroophthalmol. 2009. PMID: 19458580 Review.
-
Endovascular management of internal carotid artery injuries secondary to endonasal surgery: case series and review of the literature.J Neurosurg. 2016 Nov;125(5):1256-1276. doi: 10.3171/2015.6.JNS142483. Epub 2016 Jan 15. J Neurosurg. 2016. PMID: 26771847 Review.
Cited by
-
Imaging findings and outcomes in patients with carotid cavernous fistula at Inkosi Albert Luthuli Central Hospital in Durban.SA J Radiol. 2018 Jan 25;22(1):1264. doi: 10.4102/sajr.v22i1.1264. eCollection 2018. SA J Radiol. 2018. PMID: 31754490 Free PMC article.
-
Anatomical characteristics and morphometric analyses of the internal carotid artery using retrospective angiographic images.Surg Radiol Anat. 2023 Apr;45(4):367-374. doi: 10.1007/s00276-023-03099-7. Epub 2023 Feb 10. Surg Radiol Anat. 2023. PMID: 36763101
-
High-flow carotid cavernous fistula and the use of a microvascular plug system: initial experience.Interv Neurol. 2015 Mar;3(2):78-84. doi: 10.1159/000369477. Interv Neurol. 2015. PMID: 26019711 Free PMC article.
-
Pseudoaneurysm formation following transarterial embolization of traumatic carotid-cavernous fistula with detachable balloon: An institutional cohort long-term study.World J Radiol. 2024 Apr 28;16(4):94-108. doi: 10.4329/wjr.v16.i4.94. World J Radiol. 2024. PMID: 38690547 Free PMC article.
-
[Basilar skull fractures].Radiologe. 2021 Aug;61(8):704-709. doi: 10.1007/s00117-021-00879-3. Epub 2021 Jul 8. Radiologe. 2021. PMID: 34236447 Review. German.
References
-
- Prolo DJ, Hanberry JW. Intraluminal occlusion of a carotid cavernous sinus fistula with a balloon catheter: Technical note. J Neurosurg. 1971;35:237–242. - PubMed
-
- Parkinson D. Carotid cavernous fistula: Direct repair with preservation of the carotid. J Neurosurg. 1973;38:99–106. - PubMed
-
- Serbinento FA. Balloon catheterization and occlusion of major cerebral vessels. J Neurosurg. 1974;41:125–145. - PubMed
-
- Cervigon EC, Bien S, et al. Treatment of a recurrent traumatic carotid-cavernous fistula: Vertebro-basilar approach after surgical occlusion of the internal carotid artery. Neuroradiological. 1998;30:355–357. - PubMed
-
- Lewis AL, Tomsick TA, et al. Management of 100 consecutive direct carotid-cavernous fistulas: results of treatment with detachable balloons. Neurosurgery. 1995;36:239–245. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
