

GDC Embolisation of Cavernous Internal Carotid Artery Aneurysms with Parent Artery Preservation
- PMID: 20667207
- PMCID: PMC3679702
- DOI: 10.1177/159101990000600403
GDC Embolisation of Cavernous Internal Carotid Artery Aneurysms with Parent Artery Preservation
Abstract
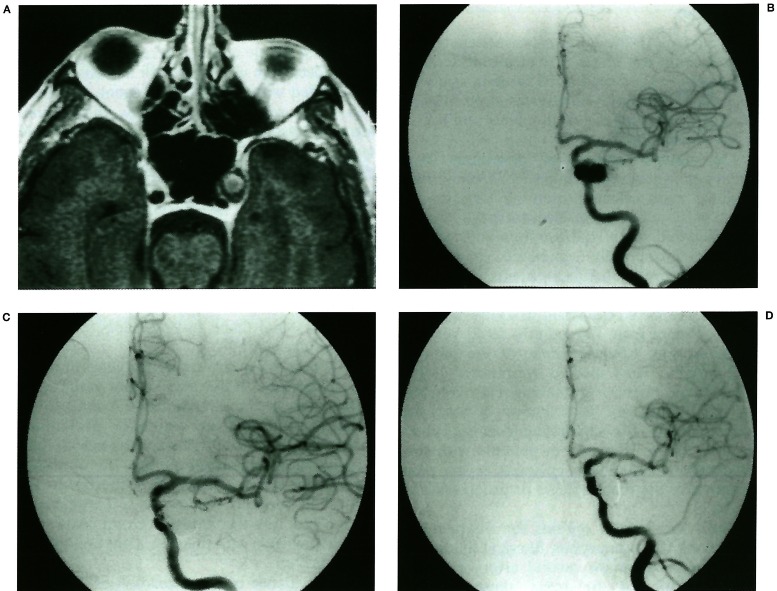
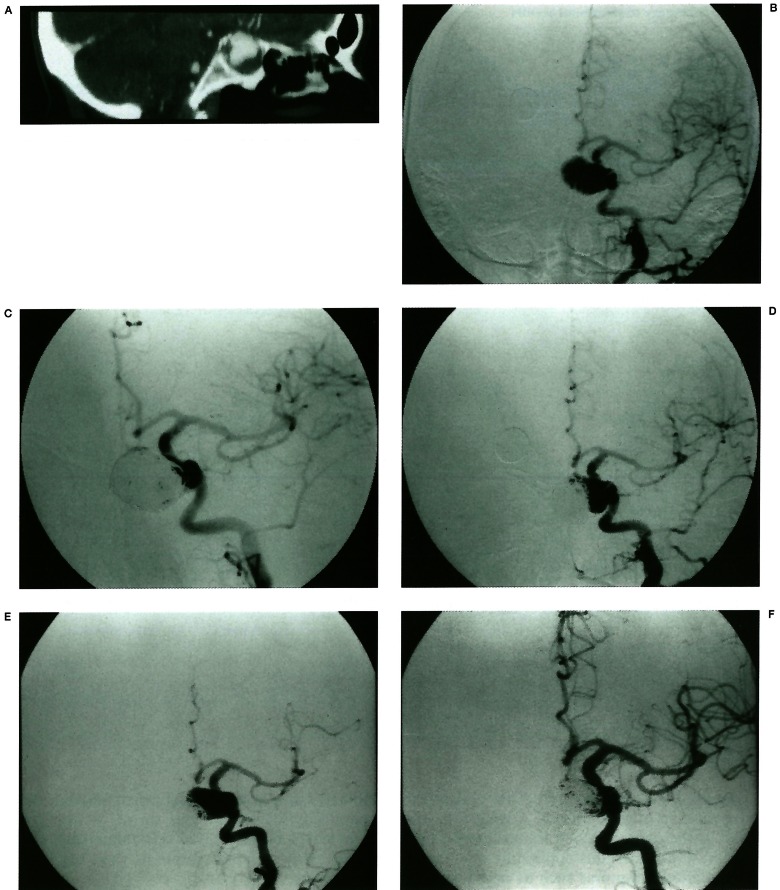
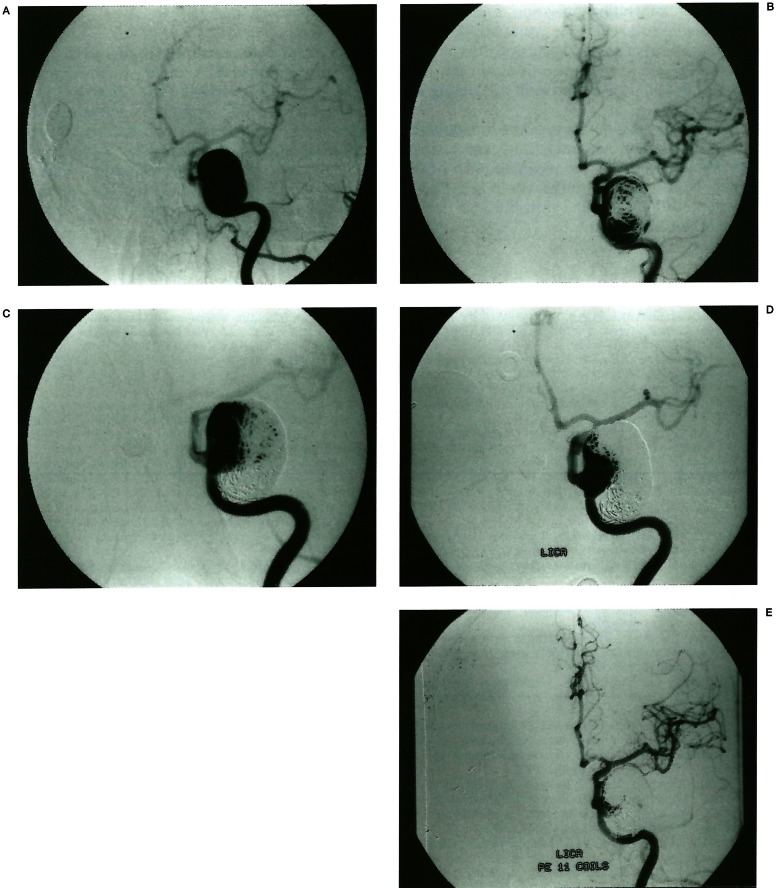
We evaluated the clinical and angiographic results of endosaccular treatment with Guglielmi detachable coils (GDCs) in 19 cases of cavernous internal carotid artery (ICA) aneurysms. The size of the aneurysms ranged from 10 to 30 mm (mean 18.4 mm) and neck size ranged from 2 to 15 mm (mean 6.7 mm). Intraluminal thrombosis was found in ten cases. Main presenting symptoms were related to mass effect in 17 cases including cranial nerve palsy, headache and vomiting. On initial GDC embolisation, total occlusion was obtained in two cases, subtotal in eight, and incomplete in nine. In two cases with incomplete occlusion, parent arteries were occluded with balloons or GDCs during or just after the procedure because of underlying diseases. A higher rate of initial occlusion was obtained in smaller and non-thrombosed aneurysms. Symptoms resolved or improved in all cases except one after initial treatment. No complication occurred related to the procedure. Follow-up angiography was obtained in 15 cases among which ten cases (66.7%) showed luminal recanalisation. Symptoms recurred in one case with luminal recanalisation. Incidence of recanalisation was similar in both large and giant aneurysms but higher in the thrombosed than non-thrombosed group. Retreatment was done in five cases with success. In conclusion, although embolisation of cavernous ICA aneurysms with GDCs was safe and effective in relieving symptoms, the incidences of initial incomplete occlusion and follow-up recanalisation were high. Therefore, we think judicious selection of the cases is necessary for endosaccular GDC embolisation in cavernous ICA aneurysms.
Figures
Similar articles
-
Midterm outcome of partially thrombosed intracranial aneurysms treated with guglielmi detachable coils.Interv Neuroradiol. 2000 Mar 30;6(1):13-25. doi: 10.1177/159101990000600103. Epub 2001 May 15. Interv Neuroradiol. 2000. PMID: 20667178 Free PMC article.
-
Internal carotid aneurysms presenting with mass effect symptoms of cranial nerve dysfunction: efficacy and imitations of endosaccular embolization with GDC.Radiat Med. 2003 Mar-Apr;21(2):80-5. Radiat Med. 2003. PMID: 12816355
-
Endovascular therapy of idiopathic cavernous aneurysms over 11 years.AJNR Am J Neuroradiol. 1998 Mar;19(3):559-65. AJNR Am J Neuroradiol. 1998. PMID: 9541319 Free PMC article.
-
Selection of cerebral aneurysms for treatment using Guglielmi detachable coils: the preliminary University of Illinois at Chicago experience.Neurosurgery. 1998 Dec;43(6):1281-95; discussion 1296-7. doi: 10.1097/00006123-199812000-00011. Neurosurgery. 1998. PMID: 9848841 Review.
-
Follow-up angiography of intracranial aneurysms treated with endovascular placement of Guglielmi detachable coils.Neurosurgery. 2002 Feb;50(2):239-49; discussion 249-50. doi: 10.1097/00006123-200202000-00003. Neurosurgery. 2002. PMID: 11844258 Review.
References
-
- Linskey M, Shekar L, et al. Aneurysms of the intracavernous caroid artery: a multidisciplinary approach. J Neurosurg. 1991;75:525–534. - PubMed
-
- Barr JD, Holmes BP, et al. Extradural aneurysms. Neuroimaging Clin North Am. 1997;7:783–802. - PubMed
-
- Fox AJ, Viñuela F, et al. Use of detachable balloons for proximal artery occlusion in the treatment of unclippable cerebral aneurysms. J Neurosurg. 1987;66:40–46. - PubMed
-
- Higashida RT, Halbach VA, et al. Endovascular detachable balloon embolization therapy of cavernous carotid artery aneurysms: results in 87 cases. J Neurosurg. 1990;72:857–863. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
