

Angiographic findings and clinical significance of the anterior and posterior spinal arteries in therapeutic parent artery occlusion for vertebral artery aneurysms
- PMID: 20667208
- PMCID: PMC3679703
- DOI: 10.1177/159101990000600404
Angiographic findings and clinical significance of the anterior and posterior spinal arteries in therapeutic parent artery occlusion for vertebral artery aneurysms
Abstract
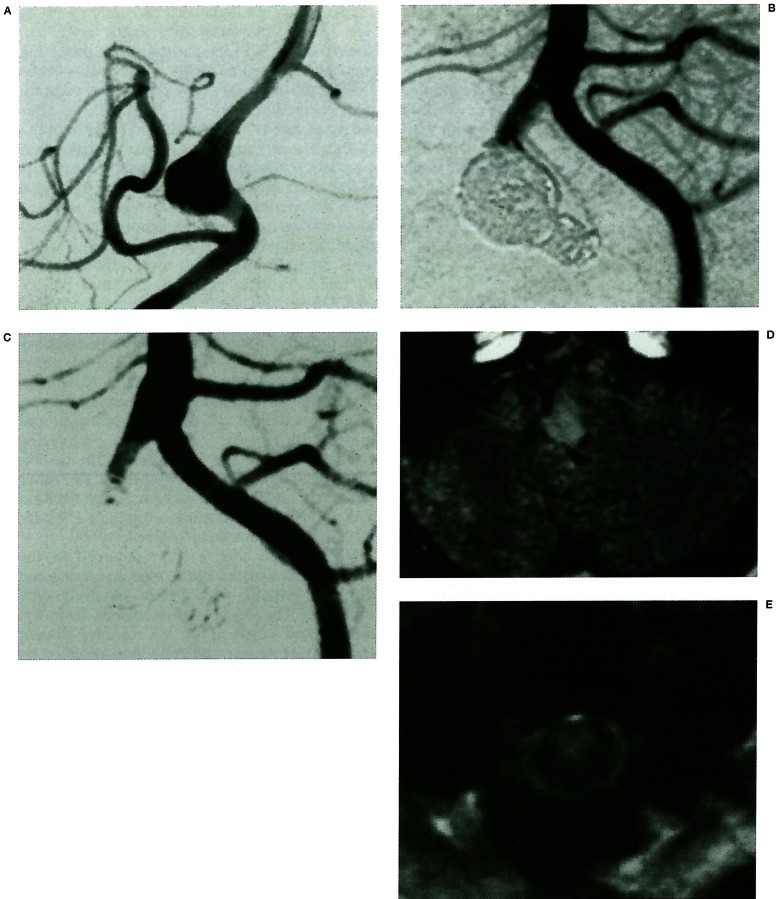
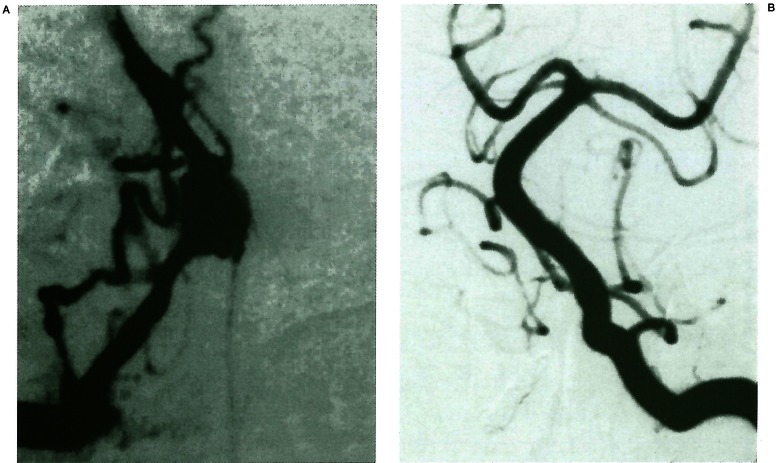
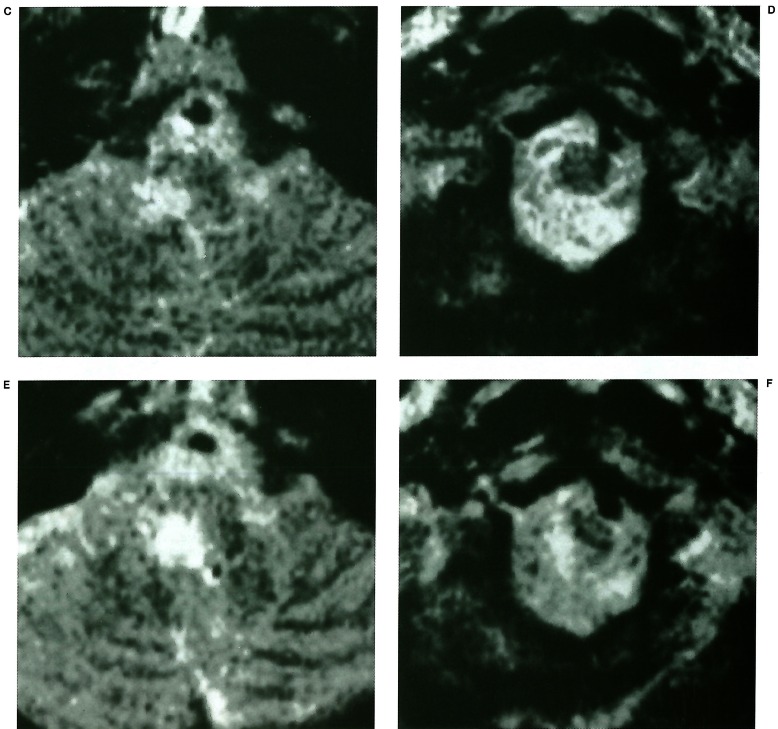
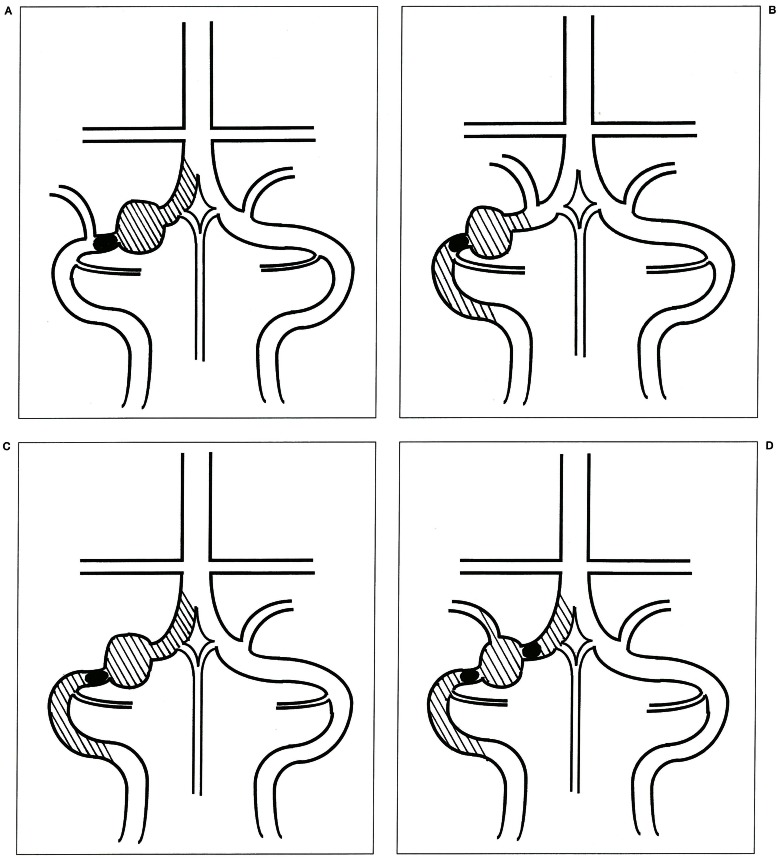
Three of 16 patients with vertebral artery (VA) aneurysms treated by parent artery occlusion suffered ischemic complications. The cause of the ischemic complications was brain stem or upper cervical spinal cord infarction due to occlusion of the anterior spinal artery (ASA), posterior spinal artery (PSA) and perforating arteries arising from the VA. Angiographic detection of ASA and PSA was studied in 71 consecutive patients (142 VAs) with various diseases who underwent digital subtraction angiography. The ASA and PSA originated from the bilateral VAs in 14% and 9%, unilateral VA in 73% and 35%, and were not detected in 13% and 56%, respectively. These results indicate that the rate of angiographic detection of the ASA originating from the bilateral VAs is considerably lower than that of previously reported anatomical studies. Special attention must be paid to the ASA, PSA and perforating arteries on preoperative vertebral angiography to prevent ischemic complications associated with therapeutic parent artery occlusion for VA aneurysms.
Figures
Similar articles
-
Severe Complications After Endovascular Trapping of Vertebral Artery Dissecting Aneurysm: Simultaneous Occurrence of Medullary and Cervical Spinal Cord Infarction.Cureus. 2022 Feb 4;14(2):e21916. doi: 10.7759/cureus.21916. eCollection 2022 Feb. Cureus. 2022. PMID: 35265433 Free PMC article.
-
Potential role of the anterior spinal artery in preventing propagation of thrombus in a therapeutically occluded vertebral artery: angiographic studies before and after endovascular treatment.Neuroradiology. 2002 Apr;44(4):347-54. doi: 10.1007/s00234-001-0734-2. Epub 2001 Dec 14. Neuroradiology. 2002. PMID: 11914814
-
Anterior spinal artery as a collateral channel in cases of bilateral vertebral arterial steno-occlusive diseases.AJNR Am J Neuroradiol. 2007 Feb;28(2):222-5. AJNR Am J Neuroradiol. 2007. PMID: 17296984 Free PMC article.
-
Radiculomedullary arterial contributions to the thoracolumbar spinal cord: an angiographic study.J Neurosurg Sci. 2023 Jun;67(3):340-343. doi: 10.23736/S0390-5616.20.05201-7. Epub 2020 Nov 30. J Neurosurg Sci. 2023. PMID: 33252207 Review.
-
Role of the Cervical Anterior Spinal Artery in the Endovascular Treatment of Vascular Diseases: Bystander, Accomplice, Victim, or Friend?Front Neurol. 2021 Oct 26;12:761006. doi: 10.3389/fneur.2021.761006. eCollection 2021. Front Neurol. 2021. PMID: 34764934 Free PMC article. Review.
Cited by
-
Discrepancy between preoperative imaging and postoperative pathological finding of ruptured intracranial dissecting aneurysm, and its surgical treatment: case report.Neurol Med Chir (Tokyo). 2014;54(3):219-26. doi: 10.2176/nmc.cr2012-0433. Epub 2013 Nov 8. Neurol Med Chir (Tokyo). 2014. PMID: 24201102 Free PMC article.
-
Severe Complications After Endovascular Trapping of Vertebral Artery Dissecting Aneurysm: Simultaneous Occurrence of Medullary and Cervical Spinal Cord Infarction.Cureus. 2022 Feb 4;14(2):e21916. doi: 10.7759/cureus.21916. eCollection 2022 Feb. Cureus. 2022. PMID: 35265433 Free PMC article.
-
Spinal cord infarction following neurointerventional procedures in the posterior cerebral circulation: a case analysis and systematic literature review.BMC Neurol. 2025 May 29;25(1):232. doi: 10.1186/s12883-025-04255-9. BMC Neurol. 2025. PMID: 40442615 Free PMC article. Review.
-
Surgical removal using V3-radial artery graft-V4 bypass and occipital artery-posterior inferior cerebellar artery bypass for a giant thrombosed aneurysm of vertebral artery compressing brain stem: Case report.Surg Neurol Int. 2019 Nov 15;10:220. doi: 10.25259/SNI_385_2019. eCollection 2019. Surg Neurol Int. 2019. PMID: 31819814 Free PMC article.
-
Microsurgical Treatment Strategy of Vertebral Artery Fusiform Aneurysm-From the Standpoint of Hemodynamic Integrity and Perforator Preservation.Front Neurol. 2021 Sep 20;12:728176. doi: 10.3389/fneur.2021.728176. eCollection 2021. Front Neurol. 2021. PMID: 34616354 Free PMC article.
References
-
- Govsa F, Aktan ZA, et al. Origin of the anterior spinal artery. Surg Radiol Anat. 1996;18:189–193. - PubMed
-
- de Oliveira E, Rhoton AL, Jr, et al. Microsurgical anatomy of the region of the foramen magnum. Surg Neurol. 1985;24:293–352. - PubMed
-
- Akar ZC, Dujovny M, et al. Microsurgical anatomy of the intracranial part of the vertebral artery. Neurol Res. 1994;16:171–180. - PubMed
-
- Krayenbühl HA, Yasargil MG. Cerebral angiography. 2nd edition. PhiladelphiaLippincott: Lippincott; 1968. pp. 141–155.
-
- Newton TH, Potts DG. Radiology of the skull and brain. book 2. Vol 2. St Louis: CV Mosby; 1974. pp. 1659–1709.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
