

Cost-effectiveness of interventions to prevent and control diabetes mellitus: a systematic review
- PMID: 20668156
- PMCID: PMC2909081
- DOI: 10.2337/dc10-0843
Cost-effectiveness of interventions to prevent and control diabetes mellitus: a systematic review
Abstract
Objective: To synthesize the cost-effectiveness (CE) of interventions to prevent and control diabetes, its complications, and comorbidities.
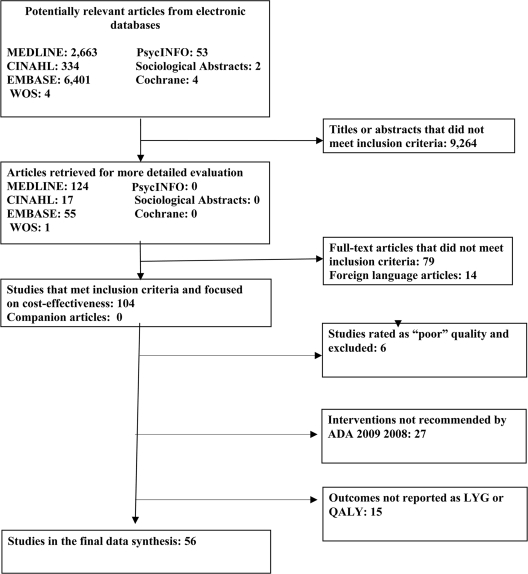
Research design and methods: We conducted a systematic review of literature on the CE of diabetes interventions recommended by the American Diabetes Association (ADA) and published between January 1985 and May 2008. We categorized the strength of evidence about the CE of an intervention as strong, supportive, or uncertain. CEs were classified as cost saving (more health benefit at a lower cost), very cost-effective (<or=$25,000 per life year gained [LYG] or quality-adjusted life year [QALY]), cost-effective ($25,001 to $50,000 per LYG or QALY), marginally cost-effective ($50,001 to $100,000 per LYG or QALY), or not cost-effective (>$100,000 per LYG or QALY). The CE classification of an intervention was reported separately by country setting (U.S. or other developed countries) if CE varied by where the intervention was implemented. Costs were measured in 2007 U.S. dollars.
Results: Fifty-six studies from 20 countries met the inclusion criteria. A large majority of the ADA recommended interventions are cost-effective. We found strong evidence to classify the following interventions as cost saving or very cost-effective: (I) Cost saving- 1) ACE inhibitor (ACEI) therapy for intensive hypertension control compared with standard hypertension control; 2) ACEI or angiotensin receptor blocker (ARB) therapy to prevent end-stage renal disease (ESRD) compared with no ACEI or ARB treatment; 3) early irbesartan therapy (at the microalbuminuria stage) to prevent ESRD compared with later treatment (at the macroalbuminuria stage); 4) comprehensive foot care to prevent ulcers compared with usual care; 5) multi-component interventions for diabetic risk factor control and early detection of complications compared with conventional insulin therapy for persons with type 1 diabetes; and 6) multi-component interventions for diabetic risk factor control and early detection of complications compared with standard glycemic control for persons with type 2 diabetes. (II) Very cost-effective- 1) intensive lifestyle interventions to prevent type 2 diabetes among persons with impaired glucose tolerance compared with standard lifestyle recommendations; 2) universal opportunistic screening for undiagnosed type 2 diabetes in African Americans between 45 and 54 years old; 3) intensive glycemic control as implemented in the UK Prospective Diabetes Study in persons with newly diagnosed type 2 diabetes compared with conventional glycemic control; 4) statin therapy for secondary prevention of cardiovascular disease compared with no statin therapy; 5) counseling and treatment for smoking cessation compared with no counseling and treatment; 6) annual screening for diabetic retinopathy and ensuing treatment in persons with type 1 diabetes compared with no screening; 7) annual screening for diabetic retinopathy and ensuing treatment in persons with type 2 diabetes compared with no screening; and 8) immediate vitrectomy to treat diabetic retinopathy compared with deferred vitrectomy.
Conclusions: Many interventions intended to prevent/control diabetes are cost saving or very cost-effective and supported by strong evidence. Policy makers should consider giving these interventions a higher priority.
Figures
References
-
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2007. Diabetes Care 2008;31:1–20 - PubMed
-
- Klonoff DC, Schwartz DM: An economic analysis of interventions for diabetes. Diabetes Care 2000;23:390–404 - PubMed
-
- Raikou M, McGuire A: The economics of screening and treatment in type 2 diabetes mellitus. Pharmacoeconomics 2003;21:543–564 - PubMed
-
- Zhang P, Engelgau MM, Norris SL, Gregg EW, Narayan KM: Application of economic analysis to Diabetes and Diabetes Care. Ann Intern Med 2004;140:972–977 - PubMed
-
- Vijgen SM, Hoogendoorn M, Baan CA, de Wit GA, Limburg W, Feenstra TL: Cost effectiveness of preventive interventions in type 2 diabetes mellitus: a systematic literature review. Pharmacoeconomics 2006;24:425–441 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
