

doi: 10.1177/159101999900500214.
Epub 2001 May 15.
Endovascular Retrograde Cortical Venous Approach to Disconnect Retrograde Leptomeningeal Venous Reflux in a Patient with Dural AVF
Affiliations
- PMID: 20670511
- PMCID: PMC4268687
- DOI: 10.1177/159101999900500214
Item in Clipboard
Endovascular Retrograde Cortical Venous Approach to Disconnect Retrograde Leptomeningeal Venous Reflux in a Patient with Dural AVF
Interv Neuroradiol.
.
Abstract
We report a case of dural arteriovenous fistual (DAVF) with cortical venous reflux in whom disconnection of the refluxing cortical vein was achieved by using a retrograde transcortical venous approach through the cortical vein itself.
Figures
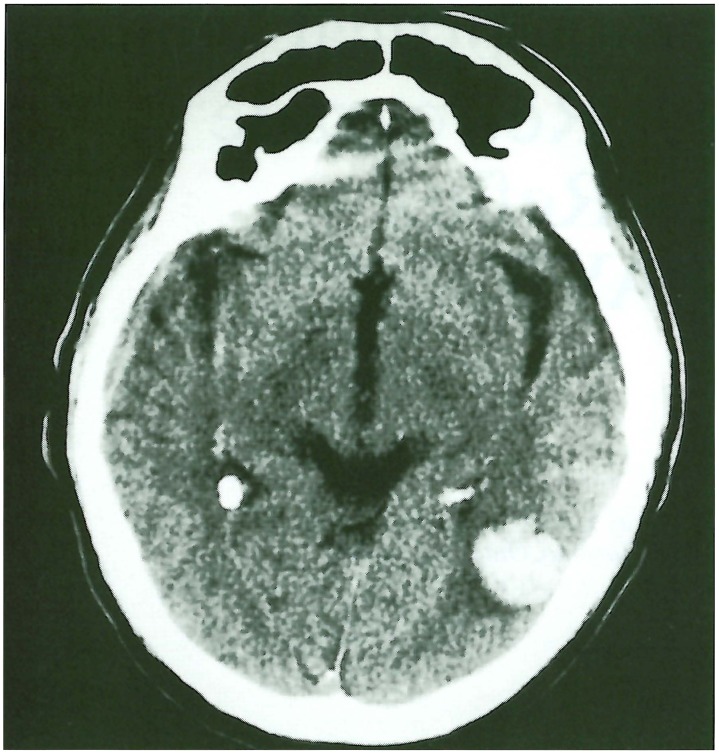
Non-contrast CT scan shows an intraparenchymal haematoma in the left temporal lobe.

MR venogram using 2D-time-of-flight technique with reconstruction of angiographic projection using MIP algorithm. The left transverse sinus is narrow and irregular (arrows).
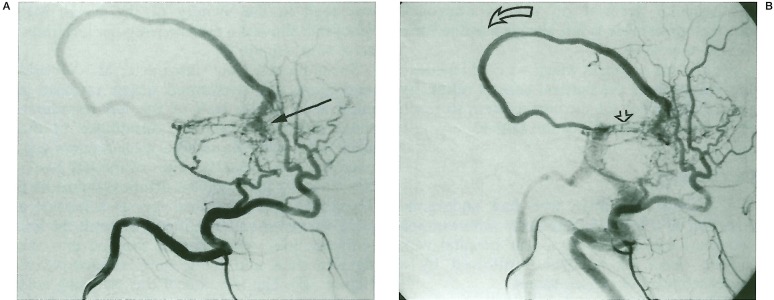
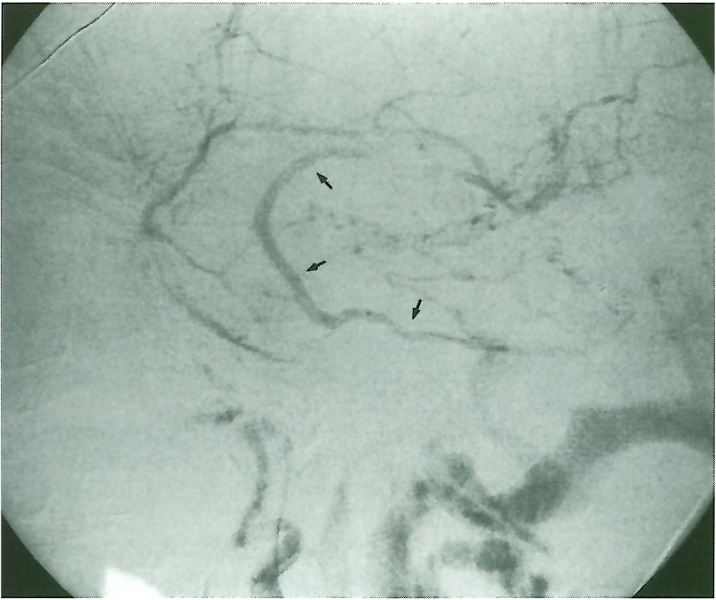
Intra-arterial angiogram, left occipital artery injection, lateral view. Multiple small feeders are seen to supply a dural AVF in the wall of the left transverse sinus (arrow). The drainage of the AVF is through a cortical vein (curved open arrow) which finally exits to the suboccipital vein after a circuitous course. Note partially thrombosed transverse sinus (straight open arrow).
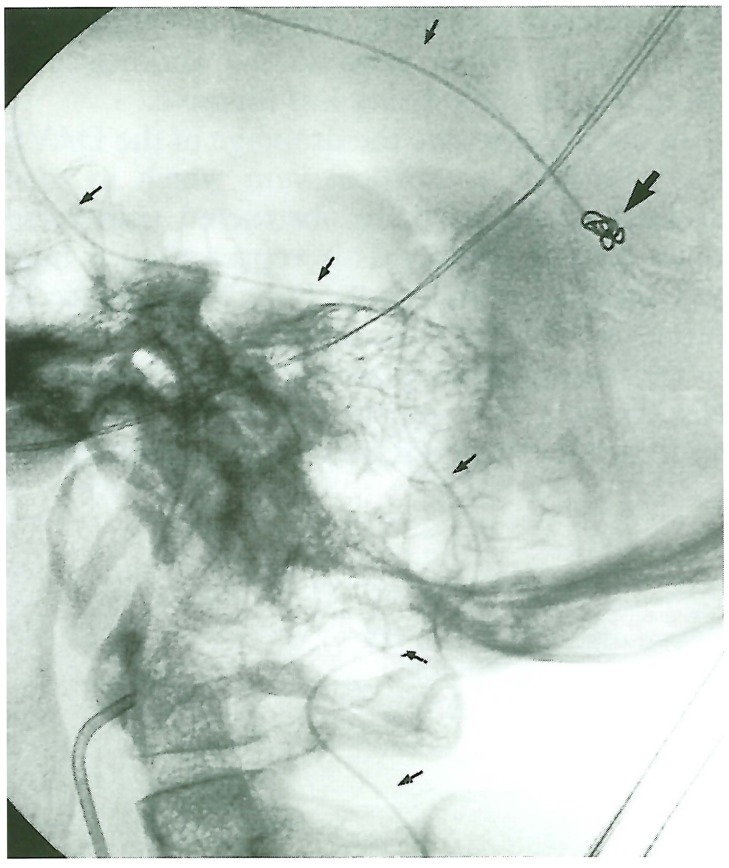
Lateral non-subtracted image showing the course of the microcatheter through the vertebral vein and retrogradely through the cortical vein (arrows). The coils were deposited adjacent to the AVF nidus. Note the presence of the arterial catheter in the left occipital artery to serve as a road map.
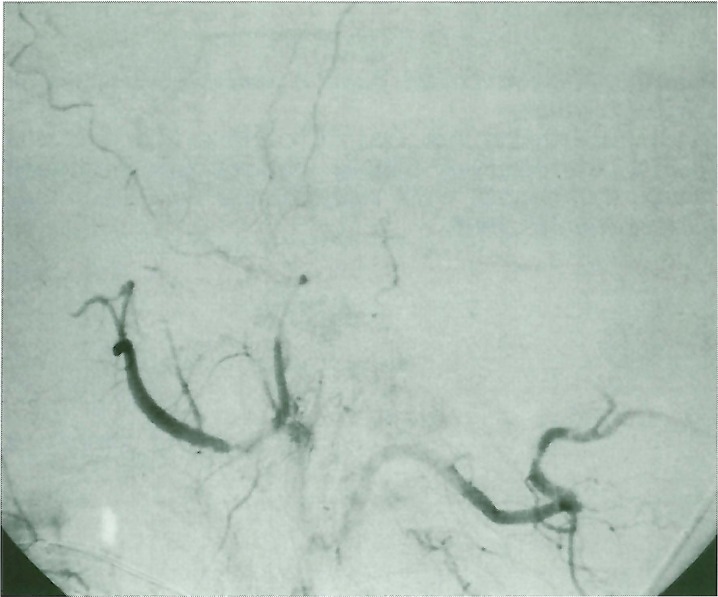
Post-procedure left external carotid artery injection, lateral view shows complete obliteration of the shunt with absence of cortical venous reflux.
Post-procedure left internal carotid artery injection, lateral view shows patency of the refluxing vein which is now draining the brain parenchyma rather than the AVF (arrows).
Similar articles
-
[Evolution of angiographic signs of venous hypertension and clinical signs of intracranial hypertension in intracranial dural arteriovenous fistulas].J Neuroradiol. 1999 Mar;26(1):49-58. J Neuroradiol. 1999. PMID: 10363442 French.
-
Endovascular treatment of sphenoid wing dural arteriovenous fistula with pure cortical venous drainage.J Stroke Cerebrovasc Dis. 2014 Jul;23(6):1730-5. doi: 10.1016/j.jstrokecerebrovasdis.2013.12.037. Epub 2014 Feb 28. J Stroke Cerebrovasc Dis. 2014. PMID: 24582791
-
Selective disconnection of cortical venous reflux as treatment for cranial dural arteriovenous fistulas.J Neurosurg. 2004 Jul;101(1):31-5. doi: 10.3171/jns.2004.101.1.0031. J Neurosurg. 2004. PMID: 15255248
-
Updates in the management of cranial dural arteriovenous fistula.Stroke Vasc Neurol. 2019 Nov 21;5(1):50-58. doi: 10.1136/svn-2019-000269. eCollection 2020. Stroke Vasc Neurol. 2019. PMID: 32411408 Free PMC article. Review.
-
Long-term outcome after endovascular treatment of cavernous sinus dural arteriovenous fistula and a literature review.Acta Neurochir (Wien). 2017 Nov;159(11):2113-2122. doi: 10.1007/s00701-017-3336-4. Epub 2017 Sep 20. Acta Neurochir (Wien). 2017. PMID: 28932918 Review.
References
-
- Davies MA, Saleh J, et al. The natural history and management of intracranial dural arteriovenous fistulae: benign lesions. Interventional Neuroradiology. 1997;3:295–302. - PubMed
-
- Davies MA, terBrugge K, et al. The natural history and management of intracranial dural arteriovenous fistulae: aggressive lesions. Interventional Neuroradiology. 1997;3:303–311. - PubMed
-
- Borden JA, Wu KW, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg. 1995;82:166–179. - PubMed
-
- Cognard C, Gobin YP, et al. Cerebral dural arteriovenous fistulas: clinical and angiographic correlation with a revised classification of venous drainage. Radiology. 1995;194:671–680. - PubMed
-
- Morris YS, Willinsky R, et al. Abstract, Annual meeting, Joint meeting of Section of Cerebrovascular Surgery and the American society of Interventional and Therapeutic Neuroradiology held at Nashville. TN: 1999. Outcome following surgical treatment of 47 aggressive (Borden type II and III) cranial dural arteriovenous fistulae; p. 73.
LinkOut - more resources
Full Text Sources
