

Thermoregulation in multiple sclerosis
- PMID: 20671034
- PMCID: PMC2980380
- DOI: 10.1152/japplphysiol.00460.2010
Thermoregulation in multiple sclerosis
Abstract
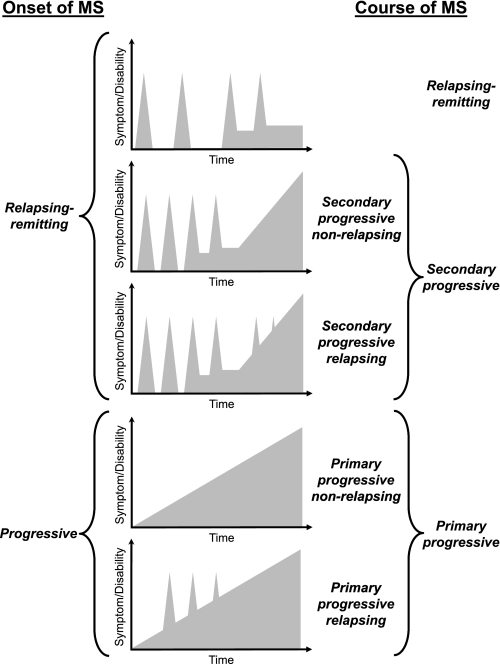
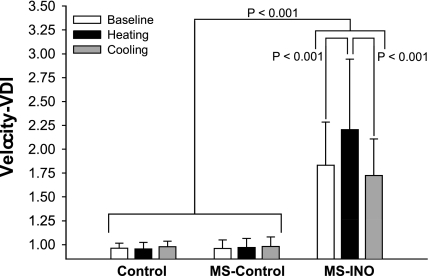
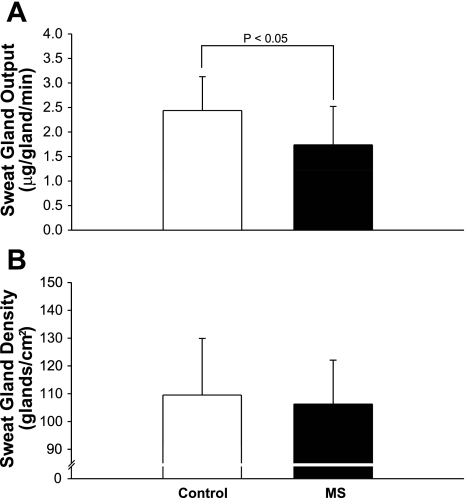
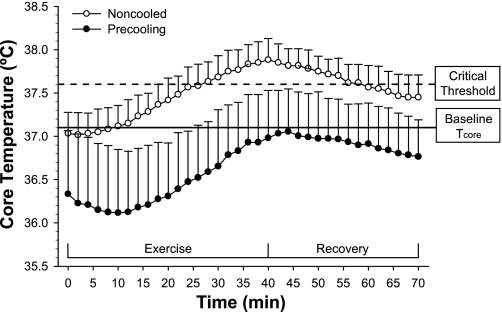
Multiple sclerosis (MS) is a progressive neurological disorder that disrupts axonal myelin in the central nervous system. Demyelination produces alterations in saltatory conduction, slowed conduction velocity, and a predisposition to conduction block. An estimated 60-80% of MS patients experience temporary worsening of clinical signs and neurological symptoms with heat exposure. Additionally, MS may produce impaired neural control of autonomic and endocrine functions. This review focuses on five main themes regarding the current understanding of thermoregulatory dysfunction in MS: 1) heat sensitivity; 2) central regulation of body temperature; 3) thermoregulatory effector responses; 4) heat-induced fatigue; and 5) countermeasures to improve or maintain function during thermal stress. Heat sensitivity in MS is related to the detrimental effects of increased temperature on action potential propagation in demyelinated axons, resulting in conduction slowing and/or block, which can be quantitatively characterized using precise measurements of ocular movements. MS lesions can also occur in areas of the brain responsible for the control and regulation of body temperature and thermoregulatory effector responses, resulting in impaired neural control of sudomotor pathways or neural-induced changes in eccrine sweat glands, as evidenced by observations of reduced sweating responses in MS patients. Fatigue during thermal stress is common in MS and results in decreased motor function and increased symptomatology likely due to impairments in central conduction. Although not comprehensive, some evidence exists concerning treatments (cooling, precooling, and pharmacological) for the MS patient to preserve function and decrease symptom worsening during heat stress.
Figures
References
-
- Andersen EB, Nordenbo AM. Sympathetic vasoconstrictor responses in multiple sclerosis with thermo-regulatory dysfunction. Clin Auton Res 7: 13–16, 1997 - PubMed
-
- Avis SP, Pryse-Phillips WE. Sudden death in multiple sclerosis associated with sun exposure: a report of two cases. Can J Neurol Sci 22: 305–307, 1995 - PubMed
-
- Bassett SW, Lake BM. Use of cold applications in the management of spasticity: report of three cases. Phys Ther Rev 38: 333–334, 1958 - PubMed
-
- Beenakker EA, Oparina TI, Hartgring A, Teelken A, Arutjunyan AV, De Keyser J. Cooling garment treatment in MS: clinical improvement and decrease in leukocyte NO production. Neurology 57: 892–894, 2001 - PubMed
-
- Bigland-Ritchie B, Woods JJ. Changes in muscle contractile properties and neural control during human muscular fatigue. Muscle Nerve 7: 691–699, 1984 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical