

Increasing cardiac contractility after myocardial infarction exacerbates cardiac injury and pump dysfunction
- PMID: 20671241
- PMCID: PMC3021375
- DOI: 10.1161/CIRCRESAHA.110.219220
Increasing cardiac contractility after myocardial infarction exacerbates cardiac injury and pump dysfunction
Erratum in
-
Correction to: Increasing Cardiac Contractility After Myocardial Infarction Exacerbates Cardiac Injury and Pump Dysfunction.Circ Res. 2020 May 8;126(10):e118. doi: 10.1161/RES.0000000000000353. Epub 2020 May 7. Circ Res. 2020. PMID: 32379570 No abstract available.
Expression of concern in
-
Expression of Concern.Circ Res. 2019 Jan 18;124(2):e4-e5. doi: 10.1161/RES.0000000000000241. Circ Res. 2019. PMID: 30582460 No abstract available.
-
Expression of Concern.Circulation. 2019 Jan 15;139(3):e5-e6. doi: 10.1161/CIR.0000000000000639. Circulation. 2019. PMID: 30615475 No abstract available.
Abstract
Rationale: Myocardial infarction (MI) leads to heart failure (HF) and premature death. The respective roles of myocyte death and depressed myocyte contractility in the induction of HF after MI have not been clearly defined and are the focus of this study.
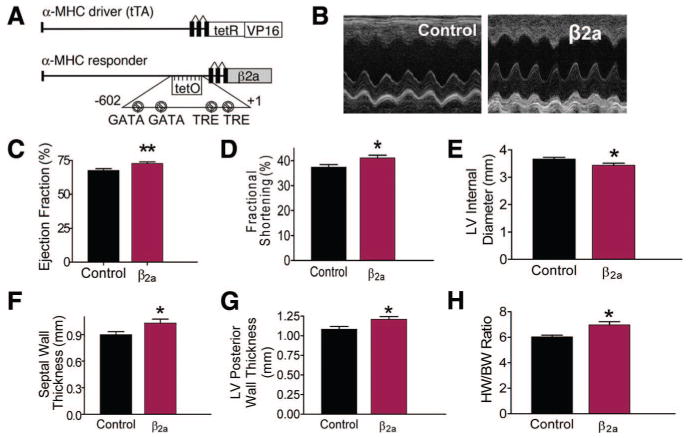
Objectives: We developed a mouse model in which we could prevent depressed myocyte contractility after MI and used it to test the idea that preventing depression of myocyte Ca(2+)-handling defects could avert post-MI cardiac pump dysfunction.
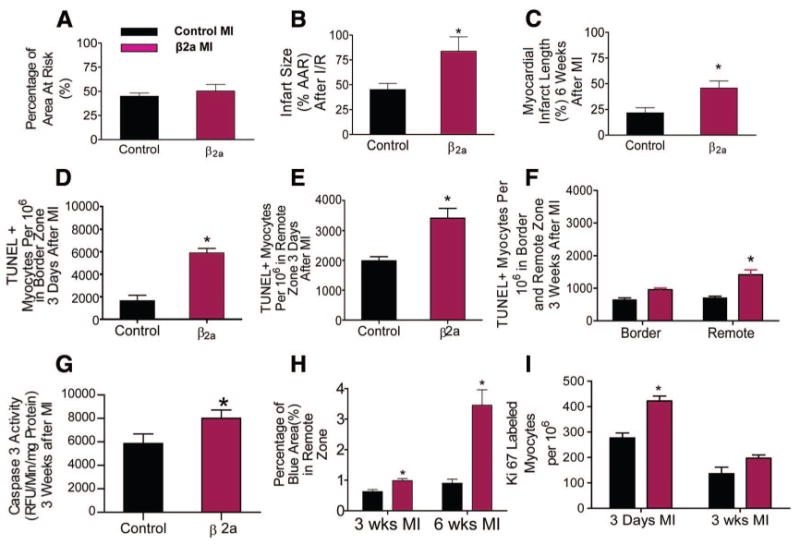
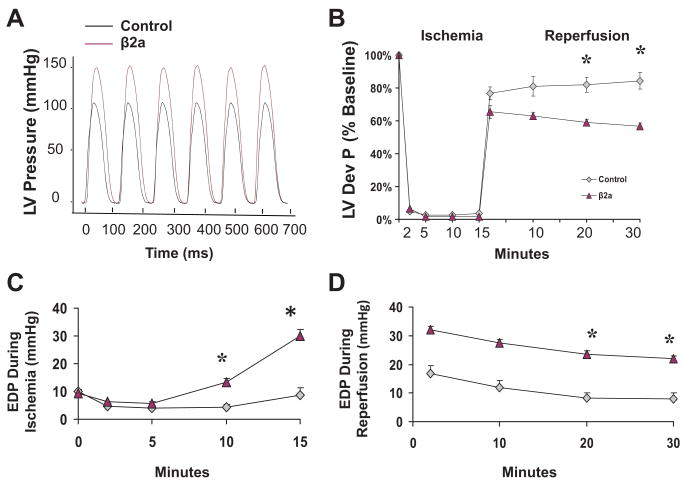
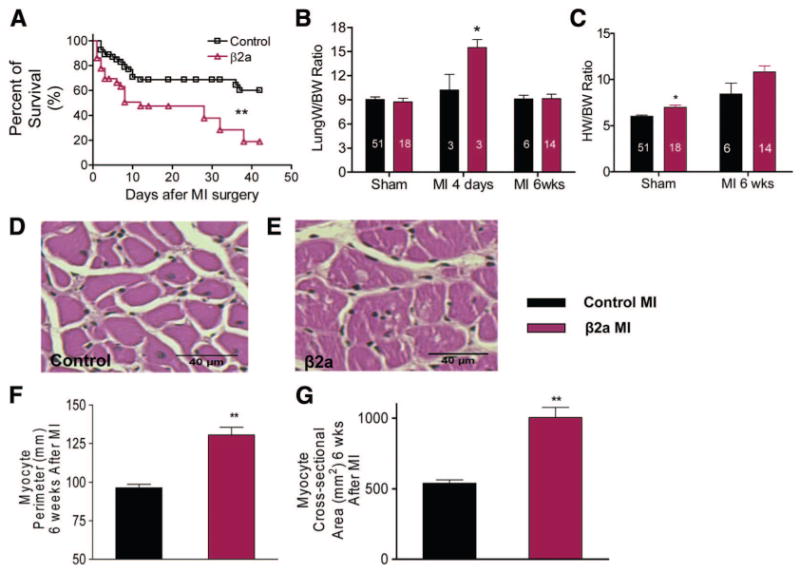
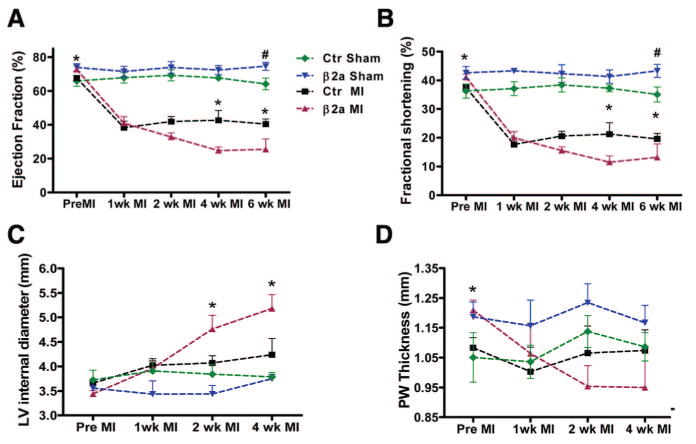
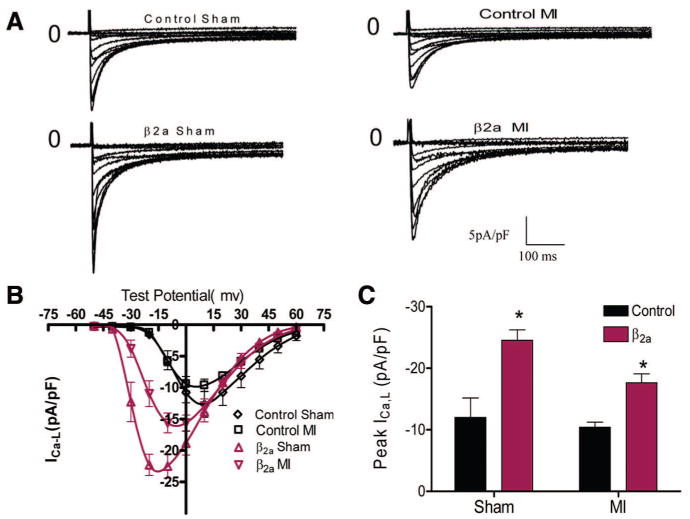
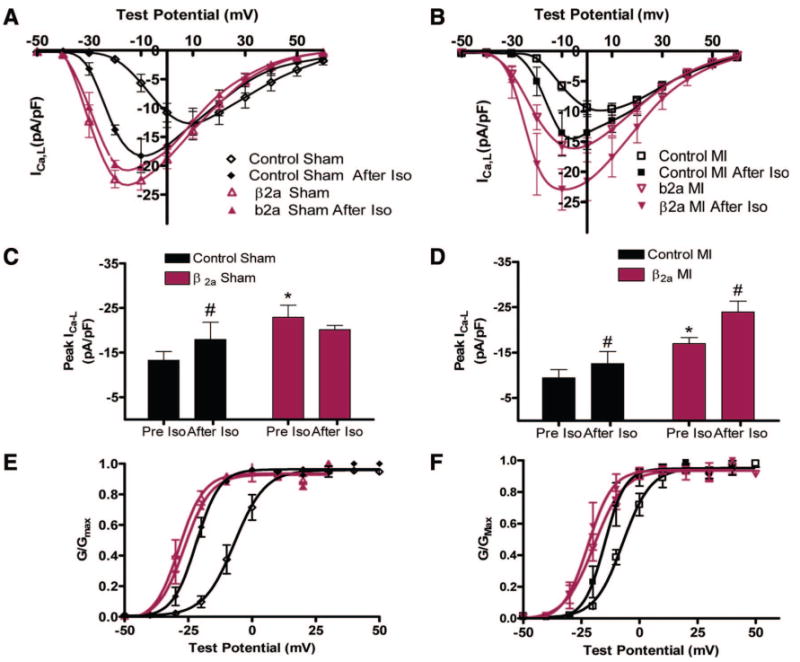
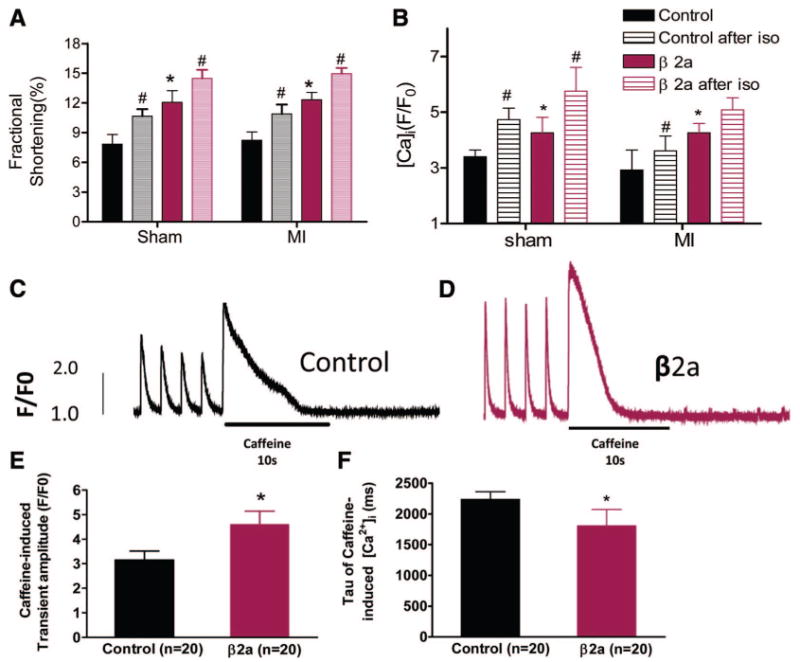
Methods and results: MI was produced in mice with inducible, cardiac-specific expression of the β2a subunit of the L-type Ca(2+) channel. Myocyte and cardiac function were compared in control and β2a animals before and after MI. β2a myocytes had increased Ca(2+) current; sarcoplasmic reticulum Ca(2+) load, contraction and Ca(2+) transients (versus controls), and β2a hearts had increased performance before MI. After MI, cardiac function decreased. However, ventricular dilation, myocyte hypertrophy and death, and depressed cardiac pump function were greater in β2a versus control hearts after MI. β2a animals also had poorer survival after MI. Myocytes isolated from β2a hearts after MI did not develop depressed Ca(2+) handling, and Ca(2+) current, contractions, and Ca(2+) transients were still above control levels (before MI).
Conclusions: Maintaining myocyte contractility after MI, by increasing Ca(2+) influx, depresses rather than improves cardiac pump function after MI by reducing myocyte number.
Figures
References
-
- Bers DM. Calcium cycling and signaling in cardiac myocytes. Annu Rev Physiol. 2008;70:23–49. - PubMed
-
- Wilkins BJ, Molkentin JD. Calcium-calcineurin signaling in the regulation of cardiac hypertrophy. Biochem Biophys Res Commun. 2004;322:1178–1191. - PubMed
-
- Gomez AM, Guatimosim S, Dilly KW, Vassort G, Lederer WJ. Heart failure after myocardial infarction: Altered excitation-contraction coupling. Circulation. 2001;104:688–693. - PubMed
-
- Houser SR, Piacentino V, III, Weisser J. Abnormalities of calcium cycling in the hypertrophied and failing heart. J Mol Cell Cardiol. 2000;32:1595–1607. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
