

Coma with Vertical Gaze Palsy: Relevance of Angio-CT in Acute Percheron Artery Syndrome
- PMID: 20671861
- PMCID: PMC2905585
- DOI: 10.1159/000315835
Coma with Vertical Gaze Palsy: Relevance of Angio-CT in Acute Percheron Artery Syndrome
Abstract
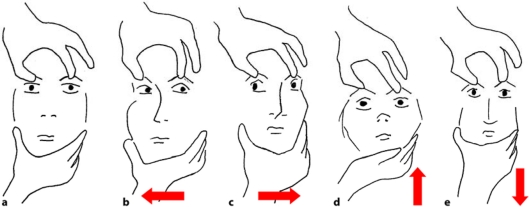
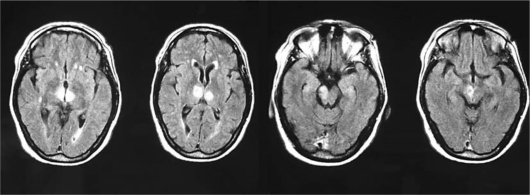
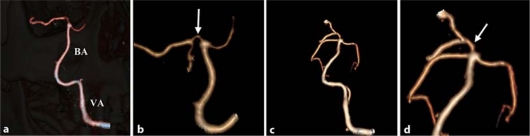
BACKGROUND: A 63-year-old woman with chronic atrial fibrillation treated with warfarin was admitted to emergency for coma and complete vertical gaze palsy. Investigations: Brain CT and MRI, echo-colour Doppler sonography of the supraaortic vessels, angio-CT of the intracranial vessels, EEG, transesophageal echocardiogram, biohumoral tests. Brain CT and MRI scans showed bilateral thalamic lesions with involvement of the right midbrain; EEG showed a diffuse alpha rhythm prevalent on the posterior regions; echo-colour Doppler sonography of the supraaortic vessels showed marked reduction of blood flow in the right vertebral artery; angio-CT scans showed occlusion of the right vertebral artery and a significant filling defect of the first part of the right posterior cerebral artery (P1) from which the artery of Percheron arises. A follow-up angio-CT showed a complete recanalization of P1. Diagnosis: Percheron artery syndrome. Treatment and Management: Aspirin, neurorehabilitation.
Figures
References
-
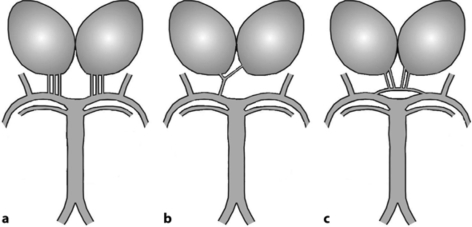
- Roitberg BZ, Tuccar E, Alp MS. Bilateral paramedian thalamic infarct in the presence of an unpaired thalamic perforating artery. Acta Neurochir (Wien) 2002;144:301–304. - PubMed
-
- Yazawa S, Kawasaki S, Kanemaru A, et al. Bilateral paramedian thalamo-midbrain infarction showing electroencephalographic alpha activity. Intern Med. 2001;40:443–448. - PubMed
-
- Kaplan HA, Ford OH. The Brain Vascular System. Amsterdam: Elsevier; 1966.
-
- Percheron G. Les artères du thalamus humain. II. Artères et territoires thalamiques paramédians de l'artère basilaire communicante. Rev Neurol (Paris) 1976;132:309–324. - PubMed
-
- Waterston JA, Stark RJ, Gilligan BS. Paramedian thalamic and midbrain infarction: the ‘mesencephalothalamic syndrome’. Clin Exp Neurol. 1987;24:45–53. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
