

Nonsteroidal anti-inflammatory drugs for wounds: pain relief or excessive scar formation?
- PMID: 20671960
- PMCID: PMC2910481
- DOI: 10.1155/2010/413238
Nonsteroidal anti-inflammatory drugs for wounds: pain relief or excessive scar formation?
Abstract
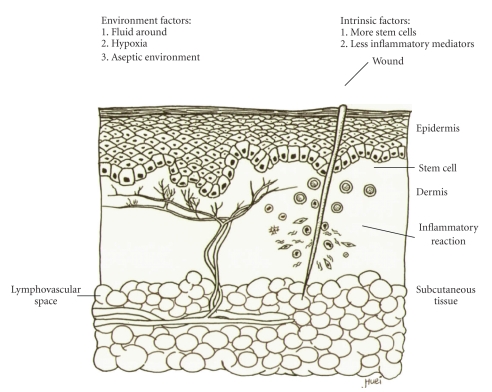
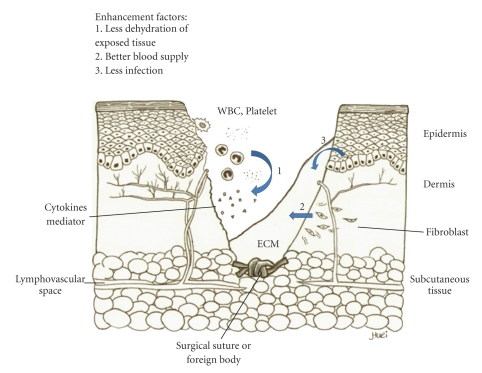
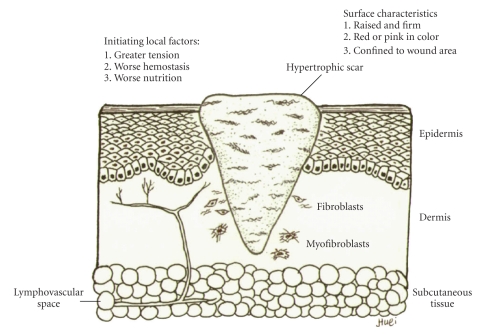
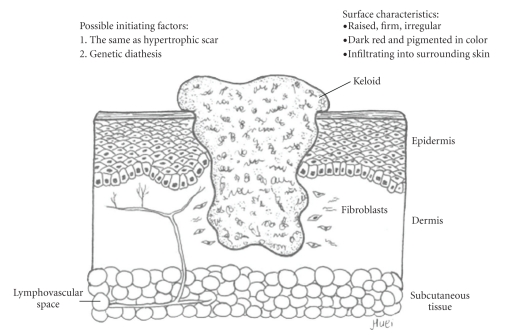
The inflammatory process has direct effects on normal and abnormal wound healing. Hypertrophic scar formation is an aberrant form of wound healing and is an indication of an exaggerated function of fibroblasts and excess accumulation of extracellular matrix during wound healing. Two cytokines--transforming growth factor-beta (TGF-beta) and prostaglandin E2 (PGE2)--are lipid mediators of inflammation involving wound healing. Overproduction of TGF-beta and suppression of PGE2 are found in excessive wound scarring compared with normal wound healing. Nonsteroidal anti-inflammatory drugs (NSAIDs) or their selective cyclooxygenase-2 (COX-2) inhibitors are frequently used as a pain-killer. However, both NSAIDs and COX-2 inhibitors inhibit PGE2 production, which might exacerbate excessive scar formation, especially when used during the later proliferative phase. Therefore, a balance between cytokines and medication in the pathogenesis of wound healing is needed. This report is a literature review pertaining to wound healing and is focused on TGF-beta and PGE2.
Figures
References
-
- Sandulache VC, Parekh A, Li-Korotky H, Dohar JE, Hebda PA. Prostaglandin E2 inhibition of keloid fibroblast migration, contraction, and transforming growth factor (TGF)-β1-induced collagen synthesis. Wound Repair and Regeneration. 2007;15(1):122–133. - PubMed
-
- Park JY, Pillinger MH, Abramson SB. Prostaglandin E2 synthesis and secretion: the role of PGE2 synthases. Clinical Immunology. 2006;119(3):229–240. - PubMed
-
- Reish RG, Eriksson E. Scar treatments: preclinical and clinical studies. Journal of the American College of Surgeons. 2008;206(4):719–730. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
