

Cervical collagen and biomechanical strength in non-pregnant women with a history of cervical insufficiency
- PMID: 20673361
- PMCID: PMC2927597
- DOI: 10.1186/1477-7827-8-92
Cervical collagen and biomechanical strength in non-pregnant women with a history of cervical insufficiency
Abstract
Background: It has been suggested that cervical insufficiency (CI) is characterized by a "muscular cervix" with low collagen and high smooth muscle concentrations also in the non-pregnant state. Therefore, the aim of this study was to investigate the biomechanical properties, collagen concentration, smooth muscle cell density, and collagen fiber orientation in cervical biopsies from non-pregnant women with a history of CI.
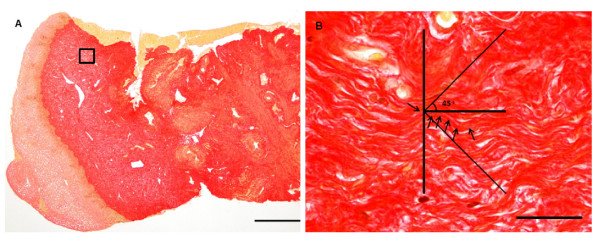
Methods: Cervical punch biopsies (2 x 15 mm) were obtained from 57 normal non-pregnant women and 22 women with a history of CI. Biomechanical tensile testing was performed, and collagen content was determined by hydroxyproline quantification. Histomorphometry was used to determine the volume densities of extracellular matrix and smooth muscle cells from the distal to the proximal part of each sample. Smooth muscle cells were identified using immunohistochemistry. Finally, collagen fiber orientation was investigated. Data are given as mean +/- SD.
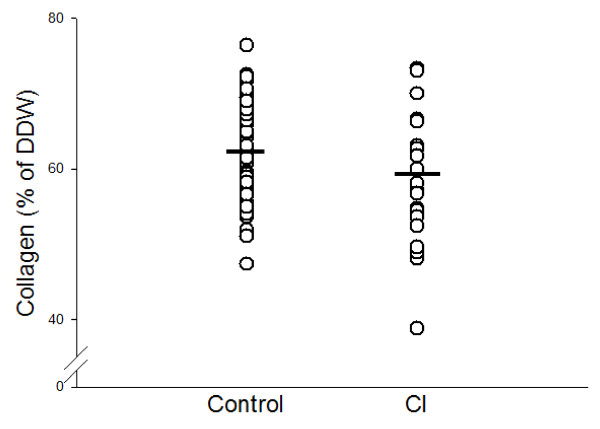
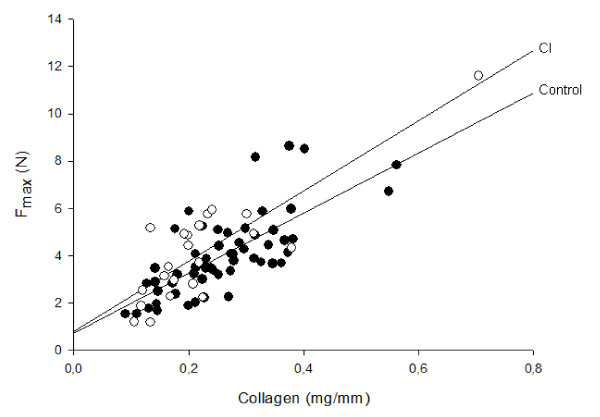
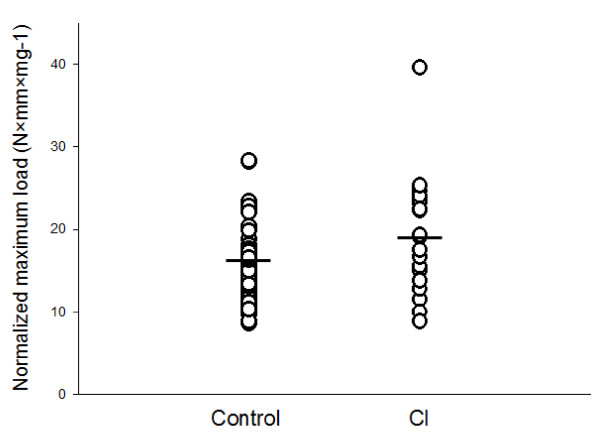
Results: Collagen concentration was lower in the CI group (58.6 +/- 8.8%) compared with the control group (62.2 +/- 6.6%) (p = 0.033). However, when data were adjusted for age and parity, no difference in collagen concentration was found between the two groups. Maximum load of the specimens did not differ between the groups (p = 0.78). The tensile strength of cervical collagen, i.e. maximum load normalized per unit collagen (mg of collagen per mm of specimen length), was increased in the CI group compared with controls (p = 0.033). No differences in the volume density of extracellular matrix or smooth muscle cells were found between the two groups. Fibers not oriented in the plane of sectioning were increased in CI patients compared with controls.
Conclusions: Cervical insufficiency does not appear to be associated with a constitutionally low collagen concentration or collagen of inferior mechanical quality. Furthermore, the hypothesis that a "muscular cervix" with an abundance of smooth muscle cells contributes to the development of cervical insufficiency is not supported by the present study.
Figures
Similar articles
-
Collagen concentration and biomechanical properties of samples from the lower uterine cervix in relation to age and parity in non-pregnant women.Reprod Biol Endocrinol. 2010 Jul 6;8:82. doi: 10.1186/1477-7827-8-82. Reprod Biol Endocrinol. 2010. PMID: 20604933 Free PMC article.
-
Cervical collagen is reduced in non-pregnant women with a history of cervical insufficiency and a short cervix.Acta Obstet Gynecol Scand. 2017 Aug;96(8):984-990. doi: 10.1111/aogs.13143. Epub 2017 May 16. Acta Obstet Gynecol Scand. 2017. PMID: 28374904
-
Cervical collagen in non-pregnant women with previous cervical incompetence.Eur J Obstet Gynecol Reprod Biol. 1996 Jul;67(1):41-5. doi: 10.1016/0301-2115(96)02440-2. Eur J Obstet Gynecol Reprod Biol. 1996. PMID: 8789748
-
In vivo characterization of the mechanics of human uterine cervices.Ann N Y Acad Sci. 2007 Apr;1101:186-202. doi: 10.1196/annals.1389.004. Epub 2007 Mar 15. Ann N Y Acad Sci. 2007. PMID: 17363446 Review.
-
A debate about ultrasound and anatomic aspects of the cervix in spontaneous preterm birth.J Med Life. 2016 Oct-Dec;9(4):342-347. J Med Life. 2016. PMID: 27928435 Free PMC article. Review.
Cited by
-
Extracellular Matrix Rigidity Modulates Human Cervical Smooth Muscle Contractility-New Insights into Premature Cervical Failure and Spontaneous Preterm Birth.Reprod Sci. 2021 Jan;28(1):237-251. doi: 10.1007/s43032-020-00268-6. Epub 2020 Jul 22. Reprod Sci. 2021. PMID: 32700284 Free PMC article.
-
Cervical alterations in pregnancy.Best Pract Res Clin Obstet Gynaecol. 2018 Oct;52:88-102. doi: 10.1016/j.bpobgyn.2018.03.007. Epub 2018 Apr 11. Best Pract Res Clin Obstet Gynaecol. 2018. PMID: 30314740 Free PMC article. Review.
-
Bioengineering and the cervix: The past, current, and future for addressing preterm birth.Curr Res Physiol. 2023 Sep 29;6:100107. doi: 10.1016/j.crphys.2023.100107. eCollection 2023. Curr Res Physiol. 2023. PMID: 38107784 Free PMC article. Review.
-
Second Harmonic Generation microscopy reveals collagen fibres are more organised in the cervix of postmenopausal women.Reprod Biol Endocrinol. 2016 Oct 21;14(1):70. doi: 10.1186/s12958-016-0204-7. Reprod Biol Endocrinol. 2016. PMID: 27769268 Free PMC article.
-
Racial and social predictors of longitudinal cervical measures: the Cervical Ultrasound Study.J Perinatol. 2017 Apr;37(4):335-339. doi: 10.1038/jp.2016.240. Epub 2017 Jan 12. J Perinatol. 2017. PMID: 28079869
References
-
- Danforth DN. The fibrous nature of the human cervix, and its relation to the isthmic segment in gravid and nongravid uteri. Am J Obstet Gynecol. 1947;53:541–557. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
