

Toward discerning the mechanisms of atrial fibrillation from surface electrocardiogram and spectral analysis
- PMID: 20673913
- PMCID: PMC2995994
- DOI: 10.1016/j.jelectrocard.2010.06.005
Toward discerning the mechanisms of atrial fibrillation from surface electrocardiogram and spectral analysis
Abstract
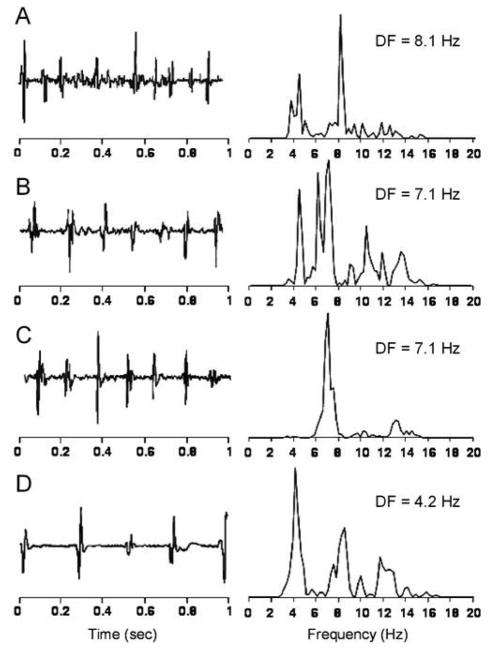
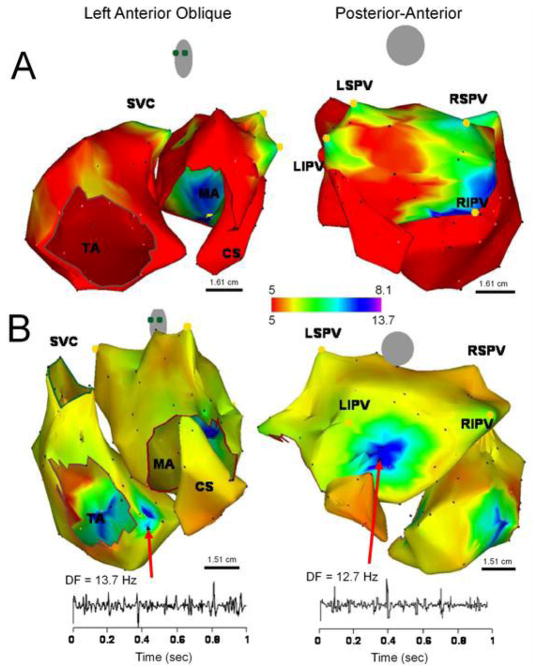
Atrial fibrillation (AF) is the main cause of stroke and the most common sustained arrhythmia, afflicting about 2.3 million Americans. Clinical treatment and management of AF would benefit from a noninvasive and global assessment of the arrhythmia; however, that avenue seems currently limited in part by our poor understanding of arrhythmia itself. Experimental studies of AF in the isolated sheep heart demonstrated that high-frequency sources in the posterior wall of the left atrium drive the fibrillatory activity throughout both atria. Motivated by those results and by a growing body of work investigating how measurements of the cycle length of activity in patients during AF can contribute to its treatment, we focused our analysis on the dispersion of dominant frequency (DF) of the activity during AF in humans. Using electroanatomic mapping and Fourier methods, we generated 3-dimensional intracardiac DF maps of the atria in patients before AF ablation procedures and identified relatively small high-DF (HDF) sites. In patients with paroxysmal AF, the HDF sites are often localized to the posterior left atrium near the ostia of the pulmonary veins. In contrast, patients with permanent AF demonstrate HDF sites that are more often localized to the atria than the posterior left atrium-pulmonary vein junction. In our study, ablation at HDF sites resulted in significant slowing of the arrhythmia and termination of sustained AF in 87% of patients with paroxysmal AF. Furthermore, we found that abolishing, by ablation, preexisting left atrium to right atrium DF gradients predicted long-term freedom of AF in both paroxysmal and persistent AF patients. Overall, the analysis of intracardiac electrical recordings in the frequency domain has greatly enhanced our understanding of its underlying mechanisms and may contribute to monitoring drug effects and guide ablation procedures aiming at its termination. On the other hand, current body surface mapping methods have also suggested better correlations between surface AF frequency and intracardiac local DFs as compared with spatiotemporal activation patterns. Therefore, further study of the correlation of spectral observables obtained from the atria and from the surface electrocardiogram during AF seems to have the potential to advance our ability to diagnose and discern mechanisms of AF noninvasively.
Copyright © 2010 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Non-invasive identification of stable rotors and focal sources for human atrial fibrillation: mechanistic classification of atrial fibrillation from the electrocardiogram.Europace. 2013 Sep;15(9):1249-58. doi: 10.1093/europace/eut038. Epub 2013 Feb 28. Europace. 2013. PMID: 23449925 Free PMC article.
-
Real-time dominant frequency analysis of the pulmonary vein in patients with paroxysmal atrial fibrillation.Pacing Clin Electrophysiol. 2012 Jan;35(1):28-37. doi: 10.1111/j.1540-8159.2011.03259.x. Epub 2011 Nov 6. Pacing Clin Electrophysiol. 2012. PMID: 22054201
-
Comparative distribution of complex fractionated atrial electrograms, high dominant frequency (HDF) sites during atrial fibrillation and HDF sites during sinus rhythm.J Interv Card Electrophysiol. 2013 Apr;36(3):297-306. doi: 10.1007/s10840-012-9748-4. Epub 2012 Nov 20. J Interv Card Electrophysiol. 2013. PMID: 23179918 Clinical Trial.
-
Ionic and substrate mechanism of atrial fibrillation: rotors and the exitación frequency approach.Arch Cardiol Mex. 2010 Oct-Dec;80(4):301-14. Arch Cardiol Mex. 2010. PMID: 21169095 Free PMC article. Review.
-
Mechanisms of atrial fibrillation: rotors, ionic determinants, and excitation frequency.Cardiol Clin. 2014 Nov;32(4):495-506. doi: 10.1016/j.ccl.2014.07.001. Epub 2014 Oct 23. Cardiol Clin. 2014. PMID: 25443232 Free PMC article. Review.
Cited by
-
Frontiers in Non-invasive Cardiac Mapping: Rotors in Atrial Fibrillation-Body Surface Frequency-Phase Mapping.Card Electrophysiol Clin. 2015 Mar 1;7(1):59-69. doi: 10.1016/j.ccep.2014.11.002. Card Electrophysiol Clin. 2015. PMID: 25729463 Free PMC article.
References
-
- Chen LY, Shen WK. Epidemiology of atrial fibrillation: a current perspective. Heart Rhythm. 2007;4:S1–S6. - PubMed
-
- Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659–666. - PubMed
-
- Haissaguerre M, Shah DC, Jais P, Hocini M, Yamane T, Deisenhofer I, Garrigue S, Clementy J. Mapping-guided ablation of pulmonary veins to cure atrial fibrillation. American Journal of Cardiology. 2000;86:9K–19K. - PubMed
-
- Moe GK, Abildskov JA. Atrial fibrillation as a self-sustaining arrhythmia independent of focal discharges. American Heart Journal. 1959;58:59–70. - PubMed
-
- Oral H, Pappone C, Chugh A, Good E, Bogun F, Pelosi F, Jr, Bates ER, Lehmann MH, Vicedomini G, Augello G, Agricola E, Sala S, Santinelli V, Morady F. Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N Engl J Med. 2006;354:934–941. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
