

Asthma in pregnancy and its pharmacologic treatment
- PMID: 20674820
- PMCID: PMC2953247
- DOI: 10.1016/j.anai.2010.05.016
Asthma in pregnancy and its pharmacologic treatment
Abstract
Background: Asthma is among the most common serious medical problems in pregnancy, and its prevalence may be increasing. Management is problematic because asthma may harm the fetus, yet little is known about fetal risks of asthma medications.
Objective: To examine the prevalence, symptom control, and pharmacologic treatment of asthma in pregnancy.
Methods: Study participants were a random sample of 3,609 mothers of nonmalformed infants born in Massachusetts between 1998 and 2006. Interviewed within 6 months of delivery, participants were asked specific asthma-related questions and classified as having physician-diagnosed, possible, past, or no asthma; those with physician-diagnosed asthma were classified as having well-controlled, not well-controlled, or poorly controlled asthma. Drug treatments were grouped into corticosteroids, beta(2)-agonists, leukotriene modifiers, combination products, and others.
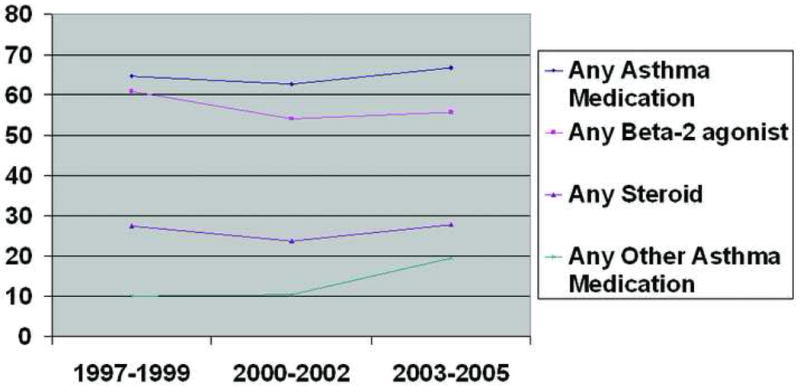
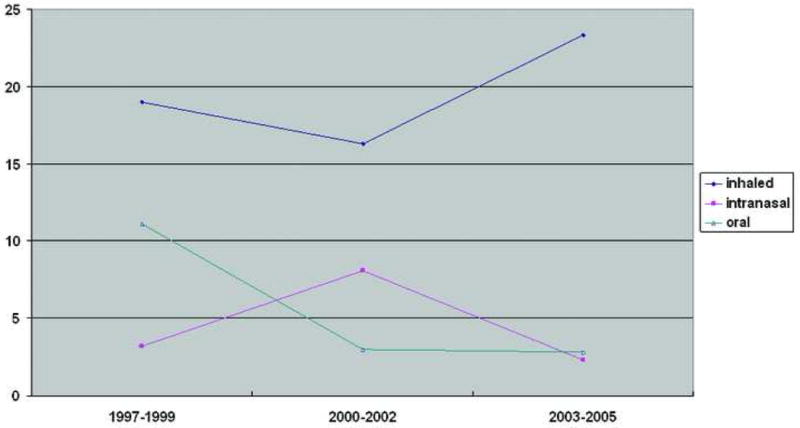
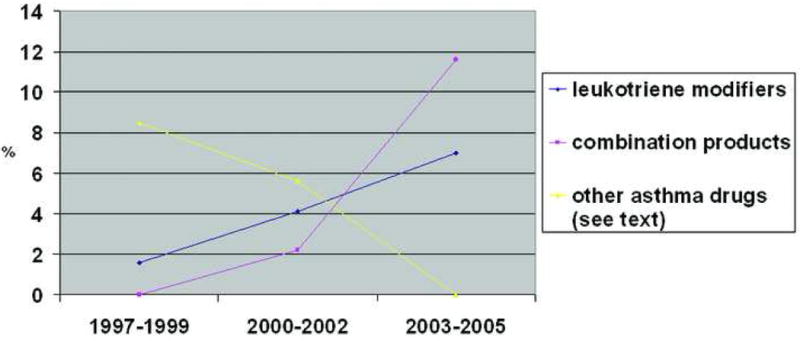
Results: Physician-diagnosed asthma was present in 502 women (13.9%) and possible asthma in an additional 578(16.0%). Higher rates of asthma were observed among women who were younger, white, obese, and less well educated, had lower income, and smoked during pregnancy. Secular changes were unremarkable: leukotriene modifiers were used by only 3.4% of asthmatic women; inhaled steroid use increased only from 19.0% during 1997-1999 to 23.3% in 2003-2005, whereas use of inhaled beta(2)-agonists exceeded 50% in both periods. Less than 40% of women with poorly controlled asthma symptoms reported use of a controller medication.
Conclusions: High rates of asthma and asthma symptoms, together with the low rates of use of controller medications, underscore the need to better understand the risks and safety of asthma medications during pregnancy.
Copyright 2010 American College of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- NAEPP expert panel report. Managing asthma during pregnancy: recommendations for pharmacologic treatment-2004 update. J Allergy Clin Immunol. 2005;115(1):34–46. - PubMed
-
- Kwon HL, Belanger K, Bracken MB. Asthma prevalence among pregnant and childbearing-aged women in the United States: estimates from national health surveys. Ann Epidemiol. 2003;13(5):317–24. - PubMed
-
- Mannino DM, Homa DM, Akinbami LJ, Moorman JE, Gwynn C, Redd SC. Surveillance for asthma--United States, 1980-1999. MMWR Surveill Summ. 2002;51(1):1–13. - PubMed
-
- Stafford RS, Ma J, Finkelstein SN, Haver K, Cockburn I. National trends in asthma visits and asthma pharmacotherapy, 1978-2002. J Allergy Clin Immunol. 2003;111(4):729–35. - PubMed
-
- Syed RZ, Zubairi AB, Zafar MA, Qureshi R. Perinatal outcomes in pregnancy with asthma. J Pak Med Assoc. 2008;58(9):525–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
