

Clinical validation of an autoantibody test for lung cancer
- PMID: 20675559
- PMCID: PMC3030465
- DOI: 10.1093/annonc/mdq361
Clinical validation of an autoantibody test for lung cancer
Abstract
Background: Autoantibodies may be present in a variety of underlying cancers several years before tumours can be detected and testing for their presence may allow earlier diagnosis. We report the clinical validation of an autoantibody panel in newly diagnosed patients with lung cancer (LC).
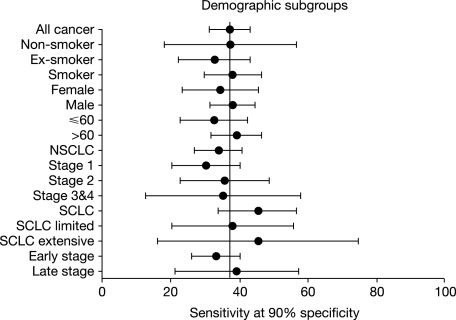
Patients and methods: Three cohorts of patients with newly diagnosed LC were identified: group 1 (n = 145), group 2 (n = 241) and group 3 (n = 269). Patients were individually matched by gender, age and smoking history to a control individual with no history of malignant disease. Serum samples were obtained after diagnosis but before any anticancer treatment. Autoantibody levels were measured against a panel of six tumour-related antigens (p53, NY-ESO-1, CAGE, GBU4-5, Annexin 1 and SOX2). Assay sensitivity was tested in relation to demographic variables and cancer type/stage.
Results: The autoantibody panel demonstrated a sensitivity/specificity of 36%/91%, 39%/89% and 37%/90% in groups 1, 2 and 3, respectively, with good reproducibility. There was no significant difference between different LC stages, indicating that the antigens included covered the different types of LC well.
Conclusion: This assay confirms the value of an autoantibody panel as a diagnostic tool and offers a potential system for monitoring patients at high risk of LC.
Figures
References
-
- Boyle P, Levin B, editors. World Cancer Report 2008. Lyon, France: IARC; 2008.
-
- Horner MJ, Ries LAG, Krapcho M, et al., editors. SEER Cancer Statistics Review, 1975–2006. Bethesda, MD: National Cancer Institute; 2009. http://seer.cancer.gov/csr/1975_2006/, based on November 2008 SEER data submission, posted to the SEER website (February 2010, date last accessed)
-
- Sone S, Takashima S, Li F, et al. Mass screening for lung cancer with mobile spiral computed tomography scanner. Lancet. 1998;351:1242–1245. - PubMed
-
- Henschke CI, McCauley DI, Yankelevitz DF, Altorki NK. Early lung cancer action project: overall design and findings from baseline screening. Lancet. 1999;354:99–105. - PubMed
-
- Swensen SJ, Jett JR, Hartman TE, et al. CT screening for lung cancer: five-year prospective experience. Radiology. 2005;235:259–265. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
