

Imaging update: acute colonic diverticulitis
- PMID: 20676257
- PMCID: PMC2780264
- DOI: 10.1055/s-0029-1236158
Imaging update: acute colonic diverticulitis
Abstract
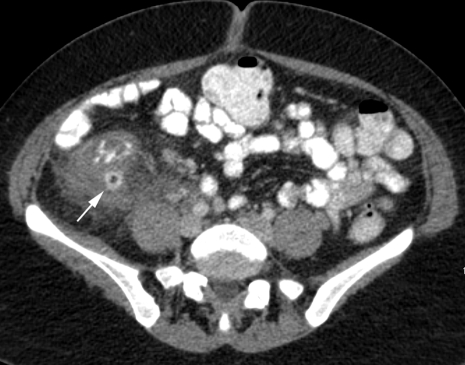
Because the incidence of colonic diverticulosis is high in the general population, incidental asymptomatic diverticulosis is commonly seen on radiology imaging studies. However, diagnostic imaging performed specifically for diverticular disease is essentially limited to imaging of suspected acute colonic diverticulitis (ACD) and its complications. The clinical diagnosis of ACD can be challenging, and imaging has become an essential tool to aid in diagnosis, assess severity of disease, and aid in treatment planning. Computed tomography (CT) has replaced contrast enema as the imaging procedure of choice for diverticulitis. Ultrasound has also been successfully used for diagnosis, and magnetic resonance imaging (MRI) has significant potential as a radiation-free imaging test for acute colonic diverticulitis.
Keywords: Acute colonic diverticulitis; computed tomography; contrast enema; diagnostic imaging; magnetic resonance imaging; ultrasound.
Figures







References
-
- Baker M E. Imaging and interventional techniques in acute left-sided diverticulitis. J Gastrointest Surg. 2008;12(8):1314–1317. - PubMed
-
- Balthazar E J, Megibow A, Schinella R A, Gordon R. Limitations in the CT diagnosis of acute diverticulitis: comparison of CT, contrast enema, and pathologic findings in 16 patients. AJR Am J Roentgenol. 1990;154(2):281–285. - PubMed
-
- Sheiman L, Levine M S, Levin A A, et al. Chronic diverticulitis: clinical, radiographic, and pathologic findings. AJR Am J Roentgenol. 2008;191(2):522–528. - PubMed
-
- Hulnick D H, Megibow A J, Balthazar E J, Gordon R B, Surapenini R, Bosniak M A. Perforated colorectal neoplasms: correlation of clinical, contrast enema, and CT examinations. Radiology. 1987;164(3):611–615. - PubMed
-
- Rao P M, Rhea J T, Novelline R A, et al. Helical CT with only colonic contrast material for diagnosing diverticulitis: prospective evaluation of 150 patients. AJR Am J Roentgenol. 1998;170(6):1445–1449. - PubMed
