

Asian blepharoplasty
- PMID: 20676313
- PMCID: PMC2884917
- DOI: 10.1055/s-0029-1224798
Asian blepharoplasty
Abstract
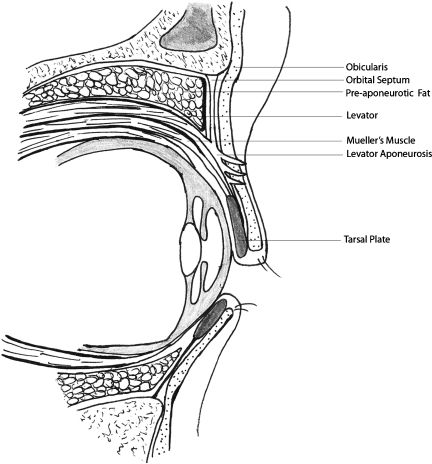
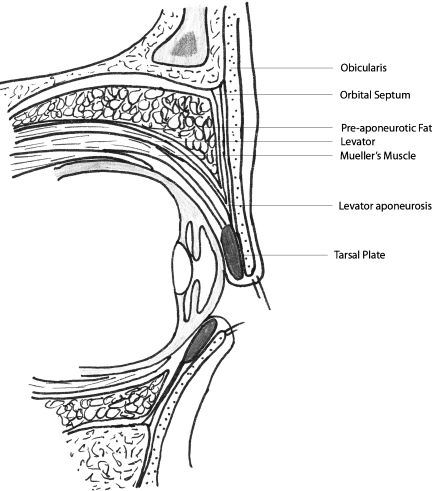
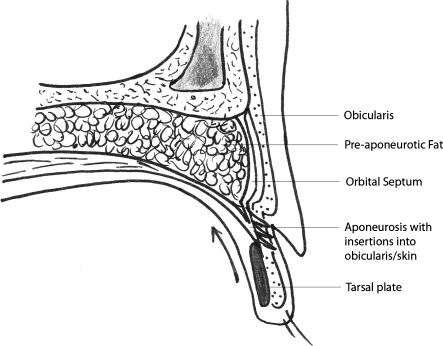
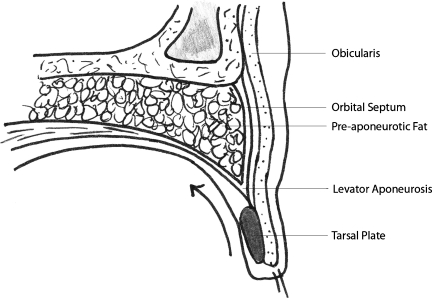
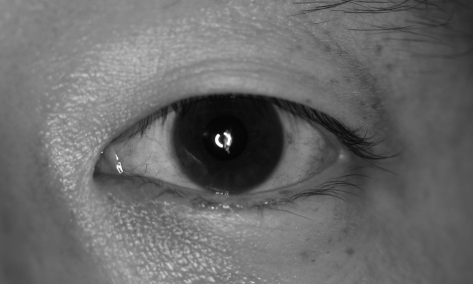
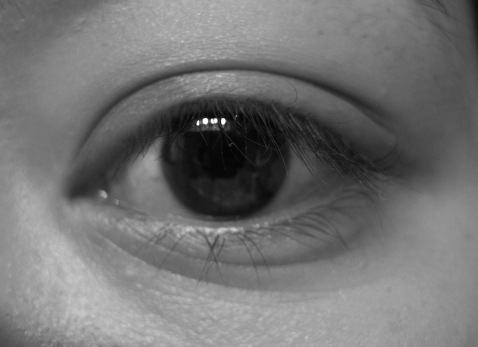
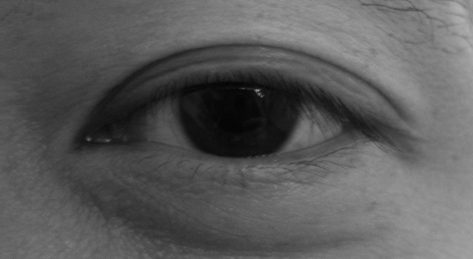
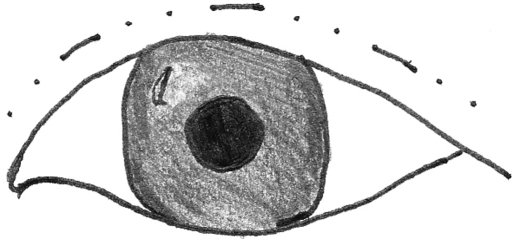
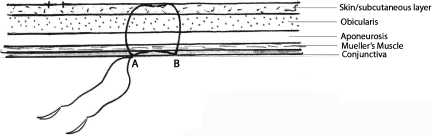
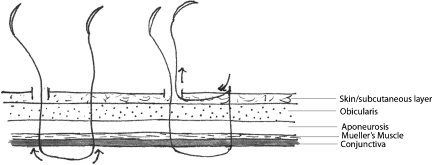
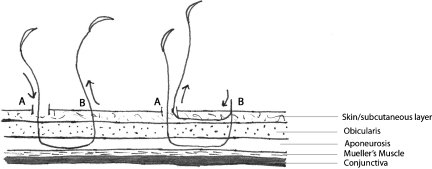
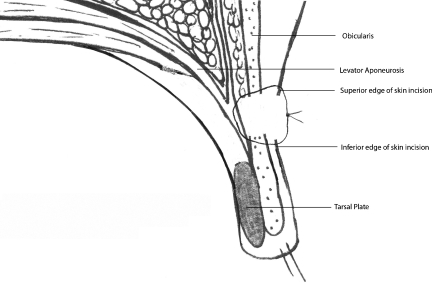
One of the defining features between an individual of Asian descent and someone of Western descent is the presence of an upper eyelid crease. Approximately 50% of Asians do not have an upper eyelid crease. The double eyelid operation, or creation of a supratarsal crease, is the most common cosmetic procedure requested in Asia and the third most common procedure requested by Asian Americans. In this comprehensive article, we explore the art of creating an eyelid crease in the individual who either does not have a crease or has an indistinct crease. We will review the history of the development of Asian blepharoplasty, explain the anatomy of the Asian eyelid and how it differs from the Caucasian eyelid, and clarify how this anatomy then translates to differences in external appearance. The two main schools of surgical techniques will be discussed along with pearls, pitfalls, and personal observations.
Keywords: Asian; blepharoplasty; double eyelid; supratarsal crease.
Figures


References
-
- Chen W PD. Asian Blepharoplasty and the Eyelid Crease. 2nd ed. New York, NY: Elsevier; 2006.
-
- McCurdy J A. Cosmetic Surgery of the Asian Face. New York, NY: Thieme Medical Publishers; 1990.
-
- Mikamo M. Plastic operation of the eyelid. J Chugaiijishimpo. 1896;17:1197.
-
- Mikamo M. Mikamo's double-eyelid operation: the advent of Japanese aesthetic surgery. 1896. Plast Reconstr Surg. 1997;99:664, discussion 664–669. - PubMed
-
- Shirakabe Y, Kinugasa T, Kawata M, Kishimoto T, Shirakabe T. The double-eyelid operation in Japan: its evolution as related to cultural changes. Ann Plast Surg. 1985;15:224–241. - PubMed
