

Non-viral causes of hepatocellular carcinoma
- PMID: 20677332
- PMCID: PMC2915420
- DOI: 10.3748/wjg.v16.i29.3603
Non-viral causes of hepatocellular carcinoma
Abstract
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy and represents an international public health concern as one of the most deadly cancers worldwide. The main etiology of HCC is chronic infection with hepatitis B and hepatitis C viruses. However, there are other important factors that contribute to the international burden of HCC. Among these are obesity, diabetes, non-alcoholic steatohepatitis and dietary exposures. Emerging evidence suggests that the etiology of many cases of HCC is in fact multifactorial, encompassing infectious etiologies, comorbid conditions and environmental exposures. Clarification of relevant non-viral causes of HCC will aid in preventative efforts to curb the rising incidence of this disease.
Figures
Comment in
-
Hepatocellular carcinoma and industrial epidemics.World J Gastroenterol. 2011 Jun 28;17(24):2976. doi: 10.3748/wjg.v17.i24.2976. World J Gastroenterol. 2011. PMID: 21734811 Free PMC article.
References
-
- El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology. 2007;132:2557–2576. - PubMed
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
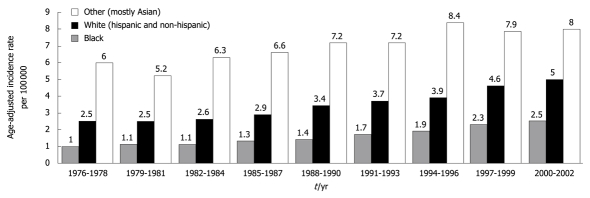
- El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med. 1999;340:745–750. - PubMed
-
- El-Serag HB, Davila JA, Petersen NJ, McGlynn KA. The continuing increase in the incidence of hepatocellular carcinoma in the United States: an update. Ann Intern Med. 2003;139:817–823. - PubMed
-
- El-Serag HB, Mason AC. Risk factors for the rising rates of primary liver cancer in the United States. Arch Intern Med. 2000;160:3227–3230. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
