

Stent-grafts placement for treatment of massive hemorrhage from ruptured hepatic artery after pancreaticoduodenectomy
- PMID: 20677346
- PMCID: PMC2915434
- DOI: 10.3748/wjg.v16.i29.3716
Stent-grafts placement for treatment of massive hemorrhage from ruptured hepatic artery after pancreaticoduodenectomy
Abstract
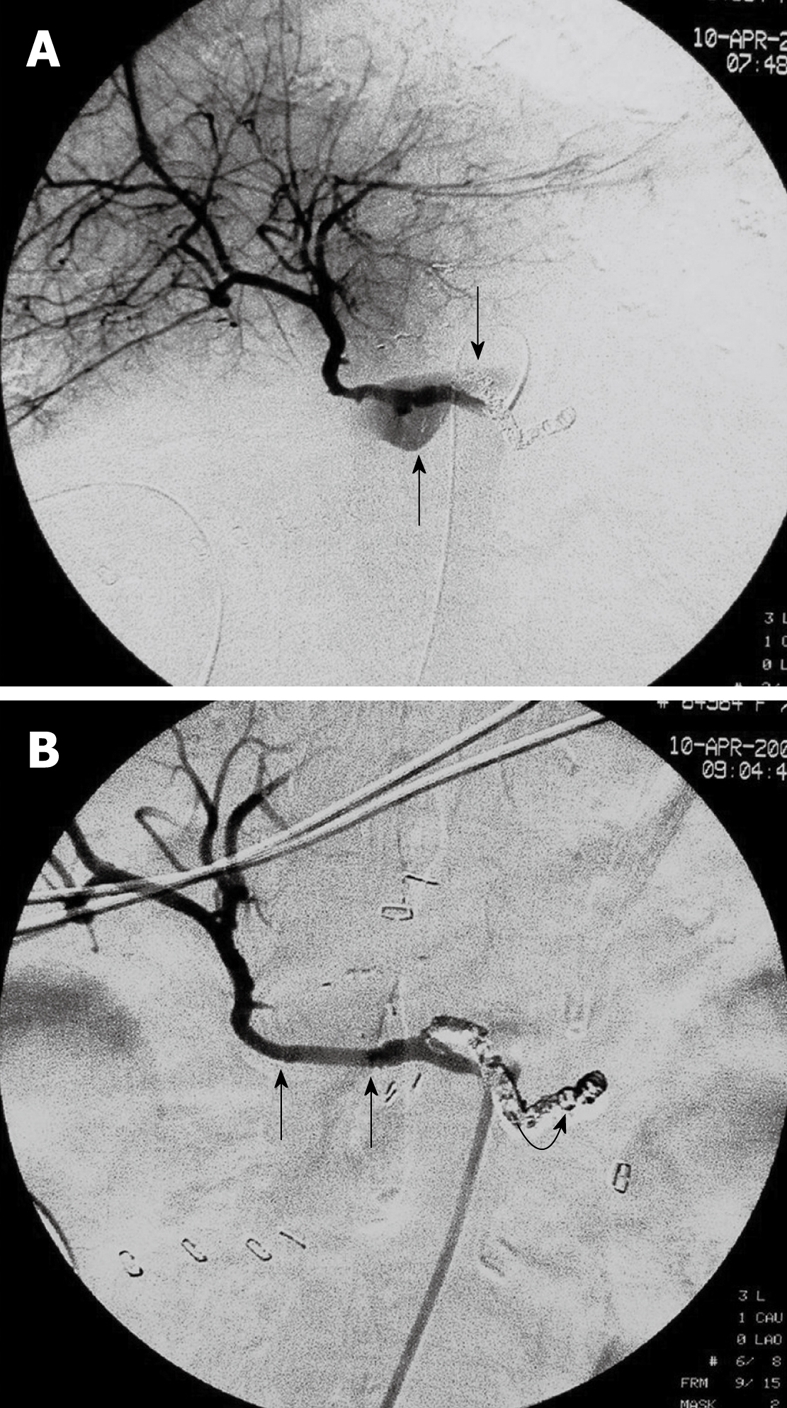
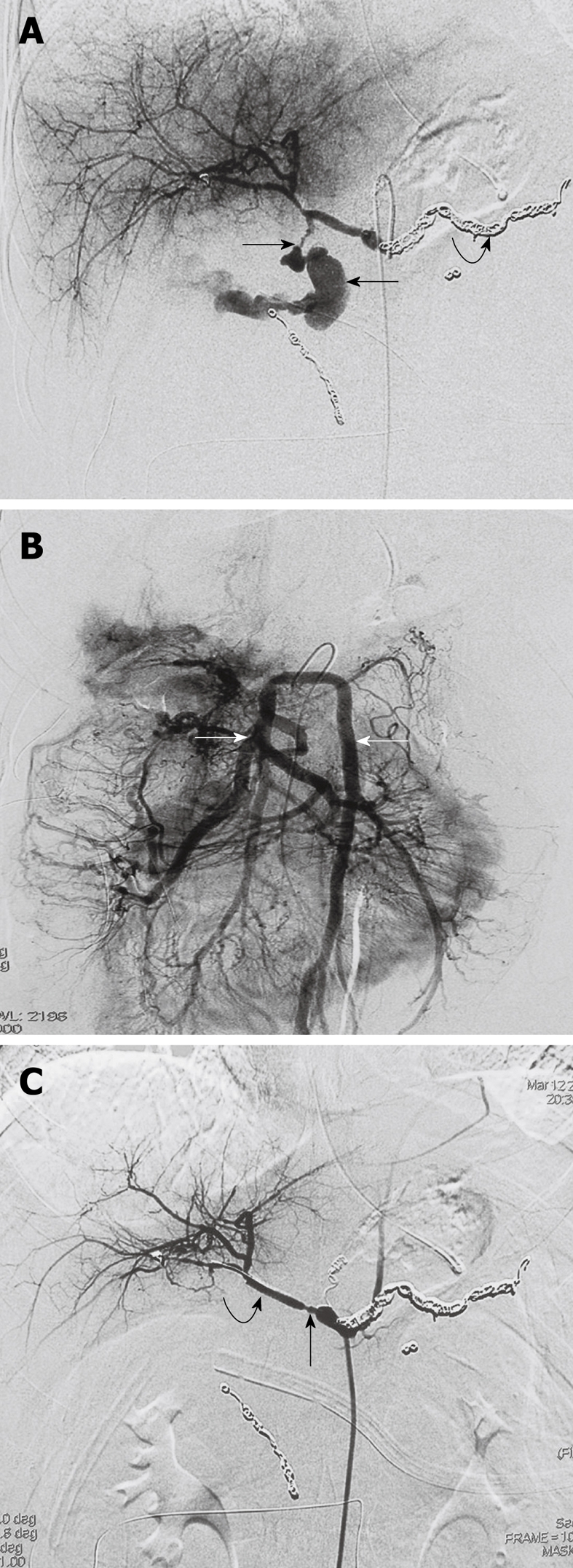
Aim: To present a series of cases with life-threatening hemorrhage from ruptured hepatic artery pseudoaneurysm after pancreaticoduodenectomy (PD) treated with placement of stent-grafts.
Methods: Massive hemorrhage from ruptured hepatic artery pseudoaneurysm after PD in 9 patients (6 men, 3 women) at the age of 23-75 years (mean 48 years), were treated with placement of percutaneous endovascular balloon-expandable coronary stent-grafts. All patients were not suitable for embolization because of a non-patent portal vein. One or more stent-grafts, ranging 3-6 mm in diameter and 16-55 mm in length, were placed to exclude ruptured pseudoaneurysm. Follow-up data, including clinical condition, liver function tests, and Doppler ultrasound examination, were recorded at the outpatient clinic.
Results: Immediate technical success was achieved in all the 9 patients. All stent-grafts were deployed in the intended position for immediate cessation of bleeding and preservation of satisfactory hepatic arterial blood flow. No significant procedure-related complications occurred. Recurrent bleeding occurred in 2 patients at 16 and 24 h, respectively, after placement of stent-grafts and treated with surgical revision. One patient died of sepsis 12 d after the interventional procedure. The remaining 6 patients were survived when they were discharged. The mean follow-up time was 10.5 mo (range 4-16 mo). No patient had recurrent bleeding after discharge. Doppler ultrasound examination verified the patency of hepatic artery and stent-grafts during the follow-up.
Conclusion: Placement of stent-grafts is an effective and safe procedure for acute life-threatening hemorrhage from ruptured hepatic artery pseudoaneurysm.
Figures
References
-
- Limongelli P, Khorsandi SE, Pai M, Jackson JE, Tait P, Tierris J, Habib NA, Williamson RC, Jiao LR. Management of delayed postoperative hemorrhage after pancreaticoduodenectomy: a meta-analysis. Arch Surg. 2008;143:1001–1007; discussion 1007. - PubMed
-
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr MG, et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery. 2007;142:20–25. - PubMed
-
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, Sarr M, Traverso W, Buchler M. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005;138:8–13. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
