

Nonoptimal lipids commonly present in young adults and coronary calcium later in life: the CARDIA (Coronary Artery Risk Development in Young Adults) study
- PMID: 20679558
- PMCID: PMC3468943
- DOI: 10.7326/0003-4819-153-3-201008030-00004
Nonoptimal lipids commonly present in young adults and coronary calcium later in life: the CARDIA (Coronary Artery Risk Development in Young Adults) study
Abstract
Background: Dyslipidemia causes coronary heart disease in middle-aged and elderly adults, but the consequences of lipid exposure during young adulthood are unclear.
Objective: To assess whether nonoptimal lipid levels during young adulthood cause atherosclerotic changes that persist into middle age.
Design: Prospective cohort study.
Setting: 4 cities in the United States.
Participants: 3258 participants from the 5115 black and white men and women recruited at age 18 to 30 years in 1985 to 1986 for the CARDIA (Coronary Artery Risk Development in Young Adults) study.
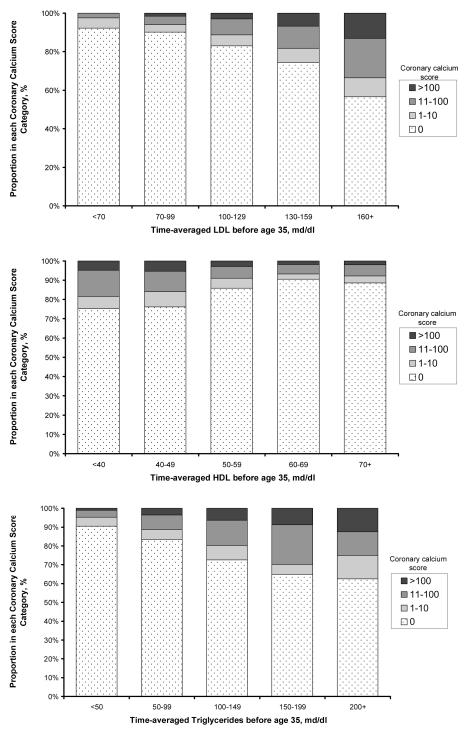
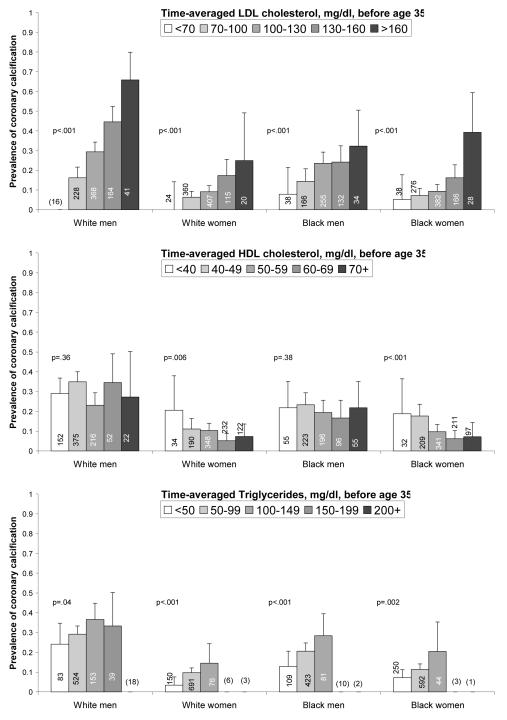
Measurements: Low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol, triglycerides, and coronary calcium. Time-averaged cumulative exposures to lipids between age 20 and 35 years were estimated by using repeated serum lipid measurements over 20 years in the CARDIA study; these measurements were then related to coronary calcium scores assessed later in life (45 years [SD, 4]).
Results: 2824 participants (87%) had nonoptimal levels of LDL cholesterol (>or=2.59 mmol/L [>or=100 mg/dL]), HDL cholesterol (<1.55 mmol/L [<60 mg/dL]), or triglycerides (>or=1.70 mmol/L [>or=150 mg/dL]) during young adulthood. Coronary calcium prevalence 2 decades later was 8% in participants who maintained optimal LDL levels (<1.81 mmol/L [<70 mg/dL]), and 44% in participants with LDL cholesterol levels of 4.14 mmol/L (160 mg/dL) or greater (P < 0.001). The association was similar across race and sex and strongly graded, with odds ratios for coronary calcium of 1.5 (95% CI, 0.7 to 3.3) for LDL cholesterol levels of 1.81 to 2.56 mmol/L (70 to 99 mg/dL), 2.4 (CI, 1.1 to 5.3) for levels of 2.59 to 3.34 mmol/L (100 to 129 mg/dL), 3.3 (CI, 1.3 to 7.8) for levels of 3.37 to 4.12 mmol/L (130 to 159 mg/dL), and 5.6 (CI, 2.0 to 16) for levels of 4.14 mmol/L (160 mg/dL) or greater, compared with levels less than 1.81 mmol/L (<70 mg/dL), after adjustment for lipid exposure after age 35 years and other coronary risk factors. Both LDL and HDL cholesterol levels were independently associated with coronary calcium after participants who were receiving lipid-lowering medications or had clinically abnormal lipid levels were excluded.
Limitation: Coronary calcium, although a strong predictor of future coronary heart disease, is not a clinical outcome.
Conclusion: Nonoptimal levels of LDL and HDL cholesterol during young adulthood are independently associated with coronary atherosclerosis 2 decades later.
Primary funding source: National Heart, Lung, and Blood Institute.
Figures
Comment in
-
Summaries for patients: Are abnormal lipid levels harmful in young adults?Ann Intern Med. 2010 Aug 3;153(3):I25. doi: 10.7326/0003-4819-153-3-201008030-00001. Ann Intern Med. 2010. PMID: 20679554 No abstract available.
-
Cardiovascular risk in young persons: secondary or primordial prevention?Ann Intern Med. 2010 Aug 3;153(3):202-3. doi: 10.7326/0003-4819-153-3-201008030-00012. Ann Intern Med. 2010. PMID: 20679564 No abstract available.
References
-
- Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) National Cholesterol Education Program, National Heart, Lung, and Blood Institute. Available at: http://www.nhlbi.nih.gov/guidelines/cholesterol/ Accessed 2/28/05, 2005.
-
- Lewington S, Whitlock G, Clarke R, Sherliker P, Emberson J, Halsey J, Qizilbash N, Peto R, Collins R. Blood cholesterol and vascular mortality by age, sex, and blood pressure: a meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet. 2007;370(9602):1829–1839. - PubMed
-
- Cholesterol Treatment Trialists’ Collaborators Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. - PubMed
-
- Anderson KM, Castelli WP, Levy D. Cholesterol and mortality. 30 years of follow-up from the Framingham study. JAMA. 1987;257(16):2176–2180. - PubMed
-
- Klag MJ, Ford DE, Mead LA, He J, Whelton PK, Liang KY, Levine DM. Serum cholesterol in young men and subsequent cardiovascular disease. N Engl J Med. 1993;328(5):313–318. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC048048/HL/NHLBI NIH HHS/United States
- N01-HC-48047/HC/NHLBI NIH HHS/United States
- N01-HC-95095/HC/NHLBI NIH HHS/United States
- N01-HC-48049/HC/NHLBI NIH HHS/United States
- N01 HC048047/HL/NHLBI NIH HHS/United States
- N01 HC048050/HL/NHLBI NIH HHS/United States
- N01-HC-48048/HC/NHLBI NIH HHS/United States
- N01 HC045204/HL/NHLBI NIH HHS/United States
- N01 HC095095/HL/NHLBI NIH HHS/United States
- N01-HC-45205/HC/NHLBI NIH HHS/United States
- N01-HC-05187/HC/NHLBI NIH HHS/United States
- N01 HC048050/HC/NHLBI NIH HHS/United States
- N01-HC-45204/HC/NHLBI NIH HHS/United States
- N01 HC048049/HL/NHLBI NIH HHS/United States
- N01-HC-48050/HC/NHLBI NIH HHS/United States
- N01 HC045205/HL/NHLBI NIH HHS/United States
- N01 HC005187/HL/NHLBI NIH HHS/United States
- N01 HC045134/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical