

Effects of methimazole on the elimination of irinotecan
- PMID: 20680278
- PMCID: PMC3016232
- DOI: 10.1007/s00280-010-1414-x
Effects of methimazole on the elimination of irinotecan
Abstract
Purpose: To study the possible pharmacokinetic and pharmacodynamic interactions between irinotecan and methimazole.
Methods: A patient treated for colorectal cancer with single agent irinotecan received methimazole co-medication for Graves' disease. Irinotecan pharmacokinetics and side effects were followed during a total of four courses (two courses with and two courses without methimazole).
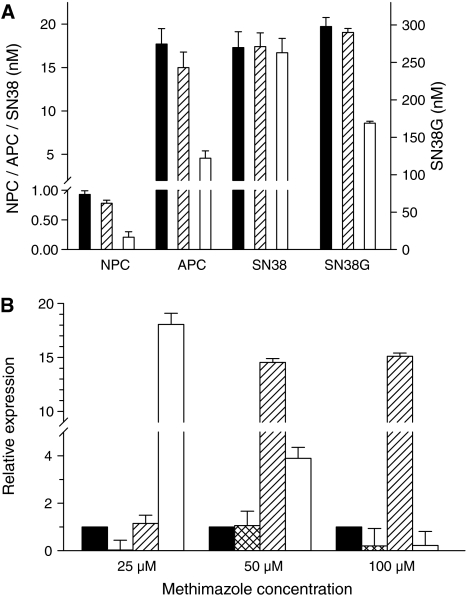
Results: Plasma concentrations of the active irinotecan metabolite SN-38 and its inactive metabolite SN-38-Glucuronide were both higher (a mean increase of 14 and 67%, respectively) with methimazole co-medication, compared to irinotecan monotherapy. As a result, the mean SN-38 glucuronidation rate increased with 47% during concurrent treatment. Other possible confounding factors did not change over time. Specific adverse events due to methimazole co-treatment were not seen.
Conclusions: Additional in vitro experiments suggest that these results can be explained by induction of UGT1A1 by methimazole, leading to higher SN-38G concentrations. The prescribed combination of these drugs may lead to highly toxic intestinal SN-38 levels. We therefore advise physicians to be very careful in combining methimazole with regular irinotecan doses, especially in patients who are prone to irinotecan toxicity.
Figures

References
-
- Vanhoefer U, Harstrick A, Achterrath W, Cao S, Seeber S, Rustum YM. Irinotecan in the treatment of colorectal cancer: clinical overview. J Clin Oncol. 2001;19:1501–1518. - PubMed
-
- Mathijssen RH, Verweij J, de Bruijn P, Loos WJ, Sparreboom A. Effects of St. John’s wort on irinotecan metabolism. J Natl Cancer Inst. 2002;94:1247–1249. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
