

Sedation confounds outcome prediction in cardiac arrest survivors treated with hypothermia
- PMID: 20680517
- PMCID: PMC3153345
- DOI: 10.1007/s12028-010-9412-8
Sedation confounds outcome prediction in cardiac arrest survivors treated with hypothermia
Abstract
Background: Therapeutic hypothermia is commonly used in comatose survivors' post-cardiopulmonary resuscitation (CPR). It is unknown whether outcome predictors perform accurately after hypothermia treatment.
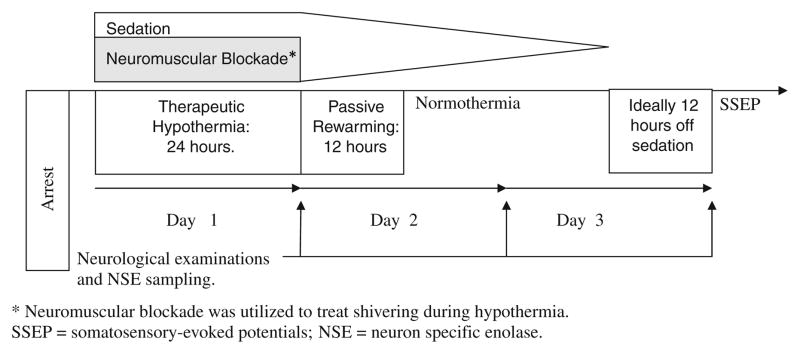
Methods: Post-CPR comatose survivors were prospectively enrolled. Six outcome predictors [pupillary and corneal reflexes, motor response to pain, and somatosensory-evoked potentials (SSEP) >72 h; status myoclonus, and serum neuron-specific enolase (NSE) levels <72 h] were systematically recorded. Poor outcome was defined as death or vegetative state at 3 months. Patients were considered "sedated" if they received any sedative drugs ≤ 12 h prior the 72 h neurological assessment.
Results: Of 85 prospectively enrolled patients, 53 (62%) underwent hypothermia. Furthermore, 53 of the 85 patients (62%) had a poor outcome. Baseline characteristics did not differ between the hypothermia and normothermia groups. Sedative drugs at 72 h were used in 62 (73%) patients overall, and more frequently in hypothermia than in normothermia patients: 83 versus 60% (P = 0.02). Status myoclonus <72 h, absent cortical responses by SSEPs >72 h, and absent pupillary reflexes >72 h predicted poor outcome with a 100% specificity both in hypothermia and normothermia patients. In contrast, absent corneal reflexes >72 h, motor response extensor or absent >72 h, and peak NSE >33 ng/ml <72 h predicted poor outcome with 100% specificity only in non-sedated patients, irrespective of prior treatment with hypothermia.
Conclusions: Sedative medications are commonly used in proximity of the 72-h neurological examination in comatose CPR survivors and are an important prognostication confounder. Patients treated with hypothermia are more likely to receive sedation than those who are not treated with hypothermia.
Figures

References
-
- Booth CM, et al. Is this patient dead, vegetative, or severely neurologically impaired? Assessing outcome for comatose survivors of cardiac arrest. JAMA. 2004;291(7):870–9. - PubMed
-
- Zheng ZJ, et al. Sudden cardiac death in the United States, 1989 to 1998. Circulation. 2001;104(18):2158–63. - PubMed
-
- Lloyd-Jones D, et al. Heart disease and stroke statistics—2010 update: a report from the American Heart Association. Circulation. 2010;121(7):e46–e215. - PubMed
-
- Peberdy MA, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58(3):297–308. - PubMed
-
- Lim C, et al. The neurological and cognitive sequelae of cardiac arrest. Neurology. 2004;63(10):1774–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
