

Risk of osteoporotic fracture in a large population-based cohort of patients with rheumatoid arthritis
- PMID: 20682035
- PMCID: PMC2945054
- DOI: 10.1186/ar3107
Risk of osteoporotic fracture in a large population-based cohort of patients with rheumatoid arthritis
Abstract
Introduction: Although osteoporosis has been reported to be more common in patients with rheumatoid arthritis (RA), little is known whether the risk of osteoporotic fractures in these patients differs by age, sex, and anatomic site.
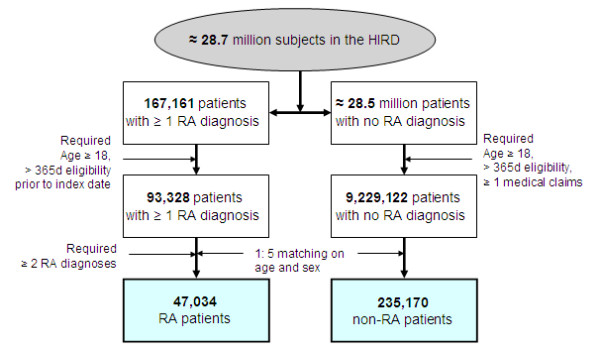
Methods: A retrospective cohort study was conducted using a health care utilization database. Incidence rates (IRs) and rate ratios (RRs) of osteoporotic fractures with 95% confidence intervals (CIs) were calculated. Multivariable Cox proportional hazards models compared the risk of osteoporotic fracture at typical sites between RA and non-RA patients.
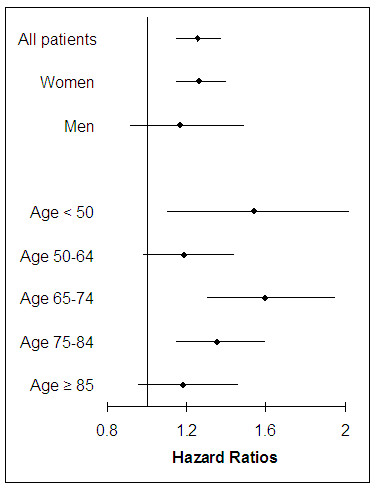
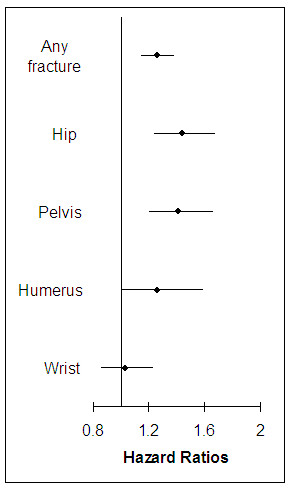
Results: During a median 1.63-year follow-up, 872 (1.9%) of 47,034 RA patients experienced a fracture. The IR for osteoporotic fracture at typical sites among RA patients was 9.6 per 1,000 person-years, 1.5 times higher than the rate of non-RA patients. The IR was highest for hip fracture (3.4 per 1,000 person-years) in RA. The IRs across all age groups were higher for women than men and increased with older age in both groups. The RRs were elevated in RA patients across all common sites of osteoporotic fracture: hip (1.62, 95% CI 1.43 to 1.84), wrist (1.15, 95% CI 1.00 to 1.32), pelvis (2.02, 95% CI 1.77 to 2.30), and humerus (1.51, 95% CI 1.27 to 1.84). After confounding adjustment, a modest increase in risk for fracture was noted with RA (hazard ratio 1.26, 95% CI 1.15 to 1.38).
Conclusions: Our study showed an increased risk of osteoporotic fractures for RA patients across all age groups, sex and various anatomic sites, compared with non-RA patients.
Figures
References
-
- Michel B, Bloch D, Wolfe F, Fries J. Fractures in rheumatoid arthritis: an evaluation of associated risk factors. J Rheumatol. 1993;20:1666–1669. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
