

Interhospital transfers among Medicare beneficiaries admitted for acute myocardial infarction at nonrevascularization hospitals
- PMID: 20682917
- PMCID: PMC3103265
- DOI: 10.1161/CIRCOUTCOMES.110.957993
Interhospital transfers among Medicare beneficiaries admitted for acute myocardial infarction at nonrevascularization hospitals
Abstract
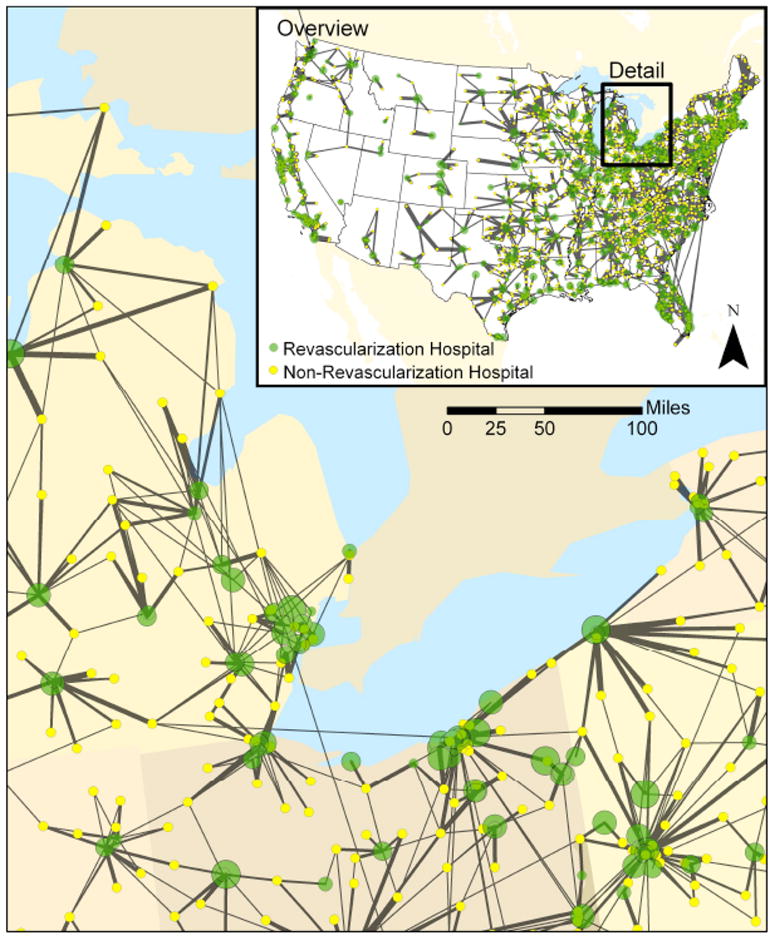
Background: Patients with acute myocardial infarction (AMI) who are admitted to hospitals without coronary revascularization are frequently transferred to hospitals with this capability, yet we know little about the basis for how such revascularization hospitals are selected.
Methods and results: We examined interhospital transfer patterns in 71 336 AMI patients admitted to hospitals without revascularization capabilities in the 2006 Medicare claims using network analysis and regression models. A total of 31 607 (44.3%) AMI patients were transferred from 1684 nonrevascularization hospitals to 1104 revascularization hospitals. Median time to transfer was 2 days. Median transfer distance was 26.7 miles, with 96.1% within 100 miles. In 45.8% of cases, patients bypassed a closer hospital to go to a farther hospital that had a better 30-day risk standardized mortality rates. However, in 36.8% of cases, another revascularization hospital with lower 30-day risk-standardized mortality was actually closer to the original admitting nonrevascularization hospital than the observed transfer destination. Adjusted regression models demonstrated that shorter transfer distances were more common than transfers to the hospitals with lowest 30-day mortality rates. Simulations suggest that an optimized system that prioritized the transfer of AMI patients to a nearby hospital with the lowest 30-day mortality rate might produce clinically meaningful reductions in mortality.
Conclusions: More than 40% of AMI patients admitted to nonrevascularization hospitals are transferred to revascularization hospitals. Many patients are not directed to nearby hospitals with the lowest 30-day risk-standardized mortality, and this may represent an opportunity for improvement.
Conflict of interest statement
Figures
Comment in
-
Moving toward improved care for the patient with ST-elevation myocardial infarction: a mandate for systems of care.Circ Cardiovasc Qual Outcomes. 2010 Sep;3(5):441-3. doi: 10.1161/CIRCOUTCOMES.110.958421. Circ Cardiovasc Qual Outcomes. 2010. PMID: 20841548 No abstract available.
References
-
- Keeley EC, Grines CL. Primary percutaneous coronary intervention for every patient with ST-segment elevation myocardial infarction: what stands in the way? Ann Intern Med. 2004;141:298–304. - PubMed
-
- Mehta RH, Stalhandske EJ, McCargar PA, Ruane TJ, Eagle KA. Elderly patients at highest risk with acute myocardial infarction are more frequently transferred from community hospitals to tertiary centers: reality or myth? Am Heart J. 1999;138:688–695. - PubMed
-
- Grines CL, Westerhausen DR, Jr, Grines LL, Hanlon JT, Logemann TL, Niemela M, Weaver WD, Graham M, Boura J, O’Neill WW, Balestrini C. A randomized trial of transfer for primary angioplasty versus on-site thrombolysis in patients with high-risk myocardial infarction: the Air Primary Angioplasty in Myocardial Infarction study. J Am Coll Cardiol. 2002;39:1713–1719. - PubMed
-
- Cantor WJ, Fitchett D, Borgundvaag B, Ducas J, Heffernan M, Cohen EA, Morrison LJ, Langer A, Dzavik V, Mehta SR, Lazzam C, Schwartz B, Casanova A, Goodman SG. Routine early angioplasty after fibrinolysis for acute myocardial infarction. N Engl J Med. 2009;360:2705–2718. - PubMed
-
- Cannon CP, Weintraub WS, Demopoulos LA, Vicari R, Frey MJ, Lakkis N, Neumann FJ, Robertson DH, DeLucca PT, DiBattiste PM, Gibson CM, Braunwald E. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001:3441879–1887. - PubMed
